Cardiovascular exercise is defined as any type of exercise that gets your heart rate up and keeps it up for a prolonged period of time. It isn’t difficult to do and there are lots of options.
Walking, jogging, running, cycling, stepping, swimming, boxercise and rowing are examples for those who haven’t suffered a stroke. Options for stroke survivors are narrowed somewhat from these choices but at least one or other of the above can probably be achievable, either supported or unsupported.
When you do these types of activities, your respiratory system starts working somewhat harder as you begin to breathe faster and more deeply. Your blood vessels expand to bring more oxygen to your muscles, and your body releases natural painkillers (endorphins).
 Your GP no doubt has already told you that if he or she could put cardiovascular exercise into a drug, it would be one of the most effective medications to prevent and/or treat patients with cardiovascular and/or cerebrovascular diseases. But cardiovascular exercise, despite the known benefits, is still known to be under-utilised by clinicians as a ‘prescription’ during rehabilitation.
Your GP no doubt has already told you that if he or she could put cardiovascular exercise into a drug, it would be one of the most effective medications to prevent and/or treat patients with cardiovascular and/or cerebrovascular diseases. But cardiovascular exercise, despite the known benefits, is still known to be under-utilised by clinicians as a ‘prescription’ during rehabilitation.
Being unfit and inactive is clearly a risk factor for stroke. But you may also have noticed that it’s a consequence of your stroke, even if you were reasonably fit pre-stroke. Being inactive for a long period of time after stroke is related to a multitude of physiological consequences that can result in reduced fitness, increased risk of cardiovascular events, sickness or even death.
The great news is that exercise training is a really potent stimulus for improving fitness after stroke and it doesn’t have to be at all onerous. It can be made to be fun and satisfying to do.

National guidelines emphasise the importance of at least 150 minutes of moderate exercise per week. Nevertheless, by the time all therapist help has finished, you may still lack a clear, results-producing, progressive programme that you can plan, perform, record and evaluate over the long term. Don’t feel guilty if you haven’t done anything much since your stroke. Let’s start the journey of putting it right.
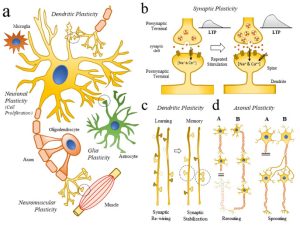
There is growing evidence to suggest cardiovascular exercise promotes neuroplasticity. In the brain, certain molecules and hormones power plasticity and cardiovascular exercise has been shown to increase how many of these molecules we have floating around in our blood. This is vital, as neuroplasticity mediates cognition and the re-learning of movement after stroke. So, not only can cardiovascular exercise increase the number of connections in your brain and improve your road to recovery, it can do so while creating a healthier cardiovascular system. Exercise also generates a boost of crucial neurochemicals in the brain as well as affecting the autonomic nervous system (ANS).
Cardiovascular exercise strengthens your heart’s efficiency. It also increases the amount of blood that leaves your heart with every beat (stroke volume), meaning your heart doesn’t have to beat as many times per minute.

Your heart essentially doesn’t have to work as hard, which in turn increases its efficiency. The increase in capillary density also allows for greater exchange of those essential nutrients your body requires. Cardiovascular exercise therefore can decrease arterial stiffness. This allows for the blood to be pushed along your arteries through proper dilation and contractibility, with an adequate amount of pressure.
Cardiovascular exercise is the first step to keeping or creating a healthy heart and arteries while the second intervention is diet. There is now a substantial body of evidence to support the importance of cardiovascular exercise for mobility, health and well-being as part of rehabilitation for stroke survivors.
Research has demonstrated that at least 80% of recurrent vascular events after an initial stroke or TIA could be prevented through cardiovascular exercise, education and lifestyle changes.
A recent systematic review has shown that exercise interventions can result in clinically meaningful blood pressure reductions, particularly if initiated early and alongside education about healthy lifestyles. The use of cardiovascular exercise to improve your heart and lung health is well established. However, of extra relevance for you is that motor control, cognition, fatigue, depression and sensory functions are all posited to improve via regular practice. Definitely worth taking some time per day to do!
 The evidence for exercise after stroke has resulted in the development of stroke-specific community exercise programmes. The system is analogous to the very well-established rehabilitation services for cardiac disease patients which usually start after usual rehabilitation has ended. Collaborations between health boards and council-run leisure centres have resulted in the establishment of exercise referral schemes, which have provided a range of stroke-specific cardiovascular exercise programmes delivered to smaller and larger groups.
The evidence for exercise after stroke has resulted in the development of stroke-specific community exercise programmes. The system is analogous to the very well-established rehabilitation services for cardiac disease patients which usually start after usual rehabilitation has ended. Collaborations between health boards and council-run leisure centres have resulted in the establishment of exercise referral schemes, which have provided a range of stroke-specific cardiovascular exercise programmes delivered to smaller and larger groups.
Additionally, some UK charities offer free or minimal-cost group exercise classes. Both modes are often well run, low in frequency (once a week for possibly one hour in duration), low in cost and usually beneficial (dependent on every possible variable, from venue accessibility to the character of the instructor).
Be careful however, not to think of such classes as the only retraining you need to do. Fitness classes can be beneficial but you’ll soon spot that those purporting to give you some rehabilitation ‘mixed in’, actually won’t be very effective at doing so. My advice would be to keep fitness and rehab efforts separate. What you need to be doing in terms of exercise is probably to regard it as comparable to a prescription of medication.
Most people end up finding it much easier and more efficient just to invest in some equipment and exercise at home daily. Stationary exercise machines such as bikes are great for this.
 Those that are known as recumbent or semi-recumbent bikes (depending how reclined it is) would be my first choice for a ‘beginner stroke survivor’. These types of gym bikes can be picked up relatively affordably from a variety of places and often aren’t cheap but they hold a considerable re-sale value.
Those that are known as recumbent or semi-recumbent bikes (depending how reclined it is) would be my first choice for a ‘beginner stroke survivor’. These types of gym bikes can be picked up relatively affordably from a variety of places and often aren’t cheap but they hold a considerable re-sale value.
You can even prop your ipad on the display ledge and watch videos or listen to music to help the pass the time. You might possibly find it difficult to keep your more-affected foot on the pedals due to weakness and/or loss of feeling and sensation in your legs. If you’re experiencing such problems, look at the internet to see if you can get a customised pedal made. This kind of job is often most efficiently carried out by a clever bicycle fixer in a dedicated bicycle shop or even a mechanic or engineer. Such people will be really great at problem-solving and coming up with the best device for you. If all else fails, it’s even possible to adhere trainers to pedals and slip your feet into them! Trainers with strong Velcro tops work well for this.
Many people will want to do some form of cardiovascular exercise daily. Go for it. If this is not achievable, it’s advised that you complete 10-60 minutes, 3-6 days per week, depending on your status and the intensity of the exercise being completed. This may sound like a lot to do, but it does need to be contemplated. And it doesn’t have to be onerous at all.
Intensity of exercise is dependent on your heart rate or the amount of effort you feel you’re exerting. The more intense the activity, the higher your heart rate will be. And the less time you’ll probably need to train for. You’ll soon find that you can create a weekly plan which allows you to slot in some frequent but short sessions of cardiovascular exercise.

How about also incorporating a variety of exercise into your lifestyle? Particularly exercises like walking and swimming, which can be done with friends or family, and are a great way to socialise while achieving some exercise. Sometimes you won’t be able to get out and about as often as you need, to do a form of exercise. So, as mentioned earlier, it’s a good idea to plan how you’re going to get it done by yourself at home.
Try to monitor yourself while exercising, so that you can follow your own progress and also know when you need to push yourself a little further. There are several ways you can do this. Heart rate monitors are a great way to keep track of the intensity you’re working at. Speak with your GP to find out what heart rate you should be working at for your age.
Pedometers are readily available and using one is simple way to monitor how many steps you do daily. A ‘wearable’, such as a FitBit, can track activity, sleep and heart rate over time, and is worth getting to provide extra real-time info.
 A big tip from Tom: make sure to record and celebrate any and all successes. Try to pinpoint how you achieved new action control in your ADLs. This is often via something achieved in your retraining. Start to become aware of these. Get this data recorded somehow.
A big tip from Tom: make sure to record and celebrate any and all successes. Try to pinpoint how you achieved new action control in your ADLs. This is often via something achieved in your retraining. Start to become aware of these. Get this data recorded somehow.
I created special training diaries to all my patients and make sure they’re completed. It makes retraining (and the planning for it) far less abstract and becomes surprisingly easy to do. These are available to buy if you want one or two, by the way, from us at the ARNI Stroke Rehab Charity – see the ARNI shopping selection
Good luck with your cardio training; please comment below if you’ve found the above helpful and tell us in your comment what you personally like to do for cardio exercise as a stroke survivor.
Have YOU got any tips and survivor ‘tricks of the trade’ you can share to help anyone reading? Gratefully received!
Much, much more info like the above can be found in the Had a Stroke? Now What? book. Get your copy from ARNI if you’ve not got yours already: all profits go straight to help stroke survivors….


 Also, note as an aside that if ‘Press’ may involve ‘where one creates’ / where/who is around to help you do stuff / what sources can you look at / involve with etc etc, it does rather shine a light on the importance of being cognisant of not just ‘where one is’ (eg, in a flat, in a tower block, in the suburbs of London) but how one can bring maximal resources to bear to help your own situation.
Also, note as an aside that if ‘Press’ may involve ‘where one creates’ / where/who is around to help you do stuff / what sources can you look at / involve with etc etc, it does rather shine a light on the importance of being cognisant of not just ‘where one is’ (eg, in a flat, in a tower block, in the suburbs of London) but how one can bring maximal resources to bear to help your own situation.
 Your brain attempts to repair as much as possible after stroke, but there is a downside. During this period of repair, the neurons that surround the infarct are not able to do their job of conducting impulses.
Your brain attempts to repair as much as possible after stroke, but there is a downside. During this period of repair, the neurons that surround the infarct are not able to do their job of conducting impulses. The more a road is used or the more popular it may become (ie, if a new short-cut to a motorway has just been loaded to the sat-nav technology), the more traffic may build suddenly up along that route, so the council may strengthen the existing road to cope with the traffic and/or add more lanes or new routes to cope with the increased traffic (new connections). It will also add speed-bumps no doubt!
The more a road is used or the more popular it may become (ie, if a new short-cut to a motorway has just been loaded to the sat-nav technology), the more traffic may build suddenly up along that route, so the council may strengthen the existing road to cope with the traffic and/or add more lanes or new routes to cope with the increased traffic (new connections). It will also add speed-bumps no doubt! Neuroplasticity allows us to compensate for irreparably damaged neural pathways by strengthening or re-routing remaining ones. The more you use these pathways, your brain will respond by upgrading them so that they’re more efficient at handling the traffic and the quicker the information is sent. The more the pathways (or ‘roads’) are used, the more adequately functional a task, ability or skill may seem to become.
Neuroplasticity allows us to compensate for irreparably damaged neural pathways by strengthening or re-routing remaining ones. The more you use these pathways, your brain will respond by upgrading them so that they’re more efficient at handling the traffic and the quicker the information is sent. The more the pathways (or ‘roads’) are used, the more adequately functional a task, ability or skill may seem to become. A big secret to success with your upper limb for example (dependent on presentation) is, after early intensive recovery efforts have moved you to a certain standard of functional movement, to start ‘creating’ things with the thought of ‘formal rehab’ firmly in the background.
A big secret to success with your upper limb for example (dependent on presentation) is, after early intensive recovery efforts have moved you to a certain standard of functional movement, to start ‘creating’ things with the thought of ‘formal rehab’ firmly in the background. And furthermore, motivation must ‘run like a ribbon’ through the creative process. This must be intrinsic to the creator – there must be a NEED to create, to problem-solve until an objective is complete. This need stokes interest, drive, enthusiasm, desire, perseverance, passion and persistence.
And furthermore, motivation must ‘run like a ribbon’ through the creative process. This must be intrinsic to the creator – there must be a NEED to create, to problem-solve until an objective is complete. This need stokes interest, drive, enthusiasm, desire, perseverance, passion and persistence.
 Dr Tom Balchin, who founded the Action for Rehabilitation from Neurological Injury (ARNI) Charity nearly 25 years ago, has been made an Officer of the British Empire (OBE) in the New Year’s Honours List.
Dr Tom Balchin, who founded the Action for Rehabilitation from Neurological Injury (ARNI) Charity nearly 25 years ago, has been made an Officer of the British Empire (OBE) in the New Year’s Honours List.  To do this required Dr Tom create what has become the only existing national accredited qualification in rehabilitation after stroke for specialist personal trainers and therapists.
To do this required Dr Tom create what has become the only existing national accredited qualification in rehabilitation after stroke for specialist personal trainers and therapists.


 Sheffield Teaching Hospitals and NHS Trusts nationally are looking for stroke survivors (aged 18+) with persistent arm weakness following an ischaemic stroke, which occurred between 6 months and 10 years ago.
Sheffield Teaching Hospitals and NHS Trusts nationally are looking for stroke survivors (aged 18+) with persistent arm weakness following an ischaemic stroke, which occurred between 6 months and 10 years ago. 





 Are between 40-80 years of age.
Are between 40-80 years of age.
 ANDREW (BY MARION). September 2024.
ANDREW (BY MARION). September 2024.

 The ‘sum of the evidence-base’ is the best we have to work with – it’s often a little out of date due to many factors, not least the nature of the time it takes to collate and display. But it’s being updated all the time. Also (I’ve found), there are very many very friendly experts in Universities who may certainly be approached in the right manner with a question or two, who will be able to refer you to online resources that may be appropriate to aid your further understanding. Ask me, if you like, and I may be able to help by asking a colleague researching in the area of your question.
The ‘sum of the evidence-base’ is the best we have to work with – it’s often a little out of date due to many factors, not least the nature of the time it takes to collate and display. But it’s being updated all the time. Also (I’ve found), there are very many very friendly experts in Universities who may certainly be approached in the right manner with a question or two, who will be able to refer you to online resources that may be appropriate to aid your further understanding. Ask me, if you like, and I may be able to help by asking a colleague researching in the area of your question. In short, as above, you need to try and understand the parameters of what you’re dealing with. This is something for when you’re now home or in other accommodation, such as your circumstances dictate.
In short, as above, you need to try and understand the parameters of what you’re dealing with. This is something for when you’re now home or in other accommodation, such as your circumstances dictate.
 Each year there are more than 100,000 first-time strokes in the UK; and as you may have heard on the news a couple of weeks ago, this number is set to rise by 50% by 2035.
Each year there are more than 100,000 first-time strokes in the UK; and as you may have heard on the news a couple of weeks ago, this number is set to rise by 50% by 2035. 
 struggling with memory issues, who may find music therapeutic and relaxing. It lets users play the piano, even if they haven’t played it in years (or ever), for free. With a library of thousands of songs, people with Alzheimer’s and dementia can use the app to access old favourite songs and unlock good memories in the process.
struggling with memory issues, who may find music therapeutic and relaxing. It lets users play the piano, even if they haven’t played it in years (or ever), for free. With a library of thousands of songs, people with Alzheimer’s and dementia can use the app to access old favourite songs and unlock good memories in the process.

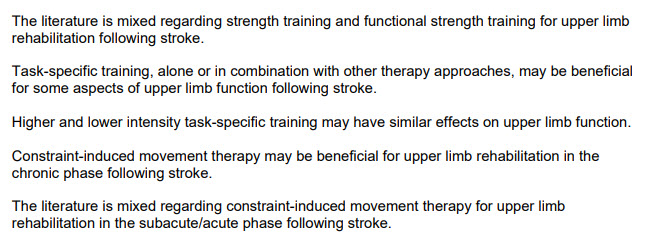
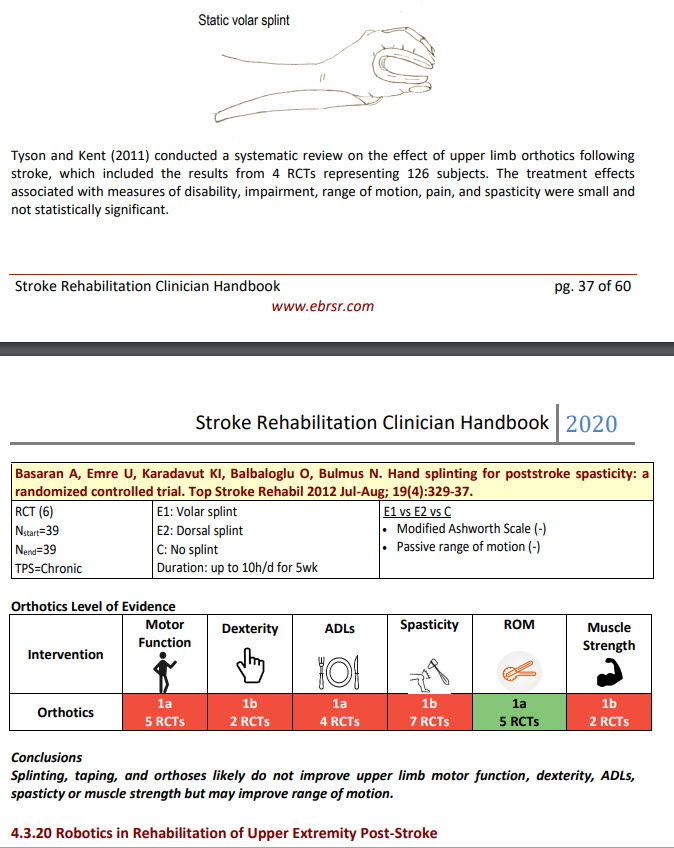
 So, overall, whether using an assistive device or not when doing re-training, ‘task-practice’ is pretty much necessary/required.
So, overall, whether using an assistive device or not when doing re-training, ‘task-practice’ is pretty much necessary/required.  Task training is critical because it will ‘force’ you to practice using your more-affected limb. This is why the Evidence-Based Review of Stroke Rehabilitation (EBRSR) concludes that constraint induced movement therapy (CIMT) in clinical settings, for those who meet the qualifying criteria, shows strong evidence of benefit in comparison to traditional therapies in the chronic stage of stroke. CIMT is a great example of task training for the upper-limb. 30 to 66 % of stroke survivors report no longer being able to use the affected arm despite trying to rehabilitate and are in danger of avoiding using it (‘learned non-use’ or inattention/ neglect of the limb). Several factors might explain this phenomenon. First, you may see no reason to try and use your bad arm and therefore remain ignorant of underlying motor potential. Second, you may not know how to use any emerging isolated movement for functional performance.
Task training is critical because it will ‘force’ you to practice using your more-affected limb. This is why the Evidence-Based Review of Stroke Rehabilitation (EBRSR) concludes that constraint induced movement therapy (CIMT) in clinical settings, for those who meet the qualifying criteria, shows strong evidence of benefit in comparison to traditional therapies in the chronic stage of stroke. CIMT is a great example of task training for the upper-limb. 30 to 66 % of stroke survivors report no longer being able to use the affected arm despite trying to rehabilitate and are in danger of avoiding using it (‘learned non-use’ or inattention/ neglect of the limb). Several factors might explain this phenomenon. First, you may see no reason to try and use your bad arm and therefore remain ignorant of underlying motor potential. Second, you may not know how to use any emerging isolated movement for functional performance.
 One great example: I created ‘DJ-Therapy’ to get my upper limb working again. I basically made up a hugely successful paradigm which was suitable for me. How I did it is all listed in
One great example: I created ‘DJ-Therapy’ to get my upper limb working again. I basically made up a hugely successful paradigm which was suitable for me. How I did it is all listed in