
 If you’ve had a stroke and like engaging with nature, Izzy and Rocksy, two friends of ARNI Stroke Rehab UK (Occupational Therapy students from the University of Southampton), would love to hear from you as they’re doing a study on how people with neurological conditions like stroke experience and engage with nature-based activities, such as gardening, outdoor walks, training in nature, conservation projects etc… please help them!
If you’ve had a stroke and like engaging with nature, Izzy and Rocksy, two friends of ARNI Stroke Rehab UK (Occupational Therapy students from the University of Southampton), would love to hear from you as they’re doing a study on how people with neurological conditions like stroke experience and engage with nature-based activities, such as gardening, outdoor walks, training in nature, conservation projects etc… please help them!
Nature-based rehabilitation (NBR) delivered as part of neurorehabilitation is a brilliant and developing approach.
To help the Southampton University students do research and create a protocol, do read on and consider doing a quick, helpful computer-based interview (no need to go anywhere) with them if you can spare the time!
The Southampton students would like to understand better, things like:
- What does nature mean to you?
- What helps or prevents you to engage with it?
- How does it support or challenge your wellbeing and daily life?
As you know, each year in the UK, around 100,000 people experience a stroke contributing to a community of approximately 1.3 million stroke survivors, more than half of whom live with a disability.
 Post-stroke fatigue is one of the most common and challenging symptoms to manage. Dong et al, (2025), reported that 45.8 % of individuals in their study experienced post-stroke fatigue, highlighting the need for interventions that address depression, improve quality of life and restore activities of daily living.
Post-stroke fatigue is one of the most common and challenging symptoms to manage. Dong et al, (2025), reported that 45.8 % of individuals in their study experienced post-stroke fatigue, highlighting the need for interventions that address depression, improve quality of life and restore activities of daily living.
Living with a neurological condition, such as stroke, involves navigating a complex mix of physical, cognitive and emotional challenges that affect everyday life, wellbeing and connection with others. Many people experience fatigue, anxiety, reduced confidence or difficulty taking part in activities that once felt meaningful.
 As interest grows in holistic, person-centred approaches to rehabilitation, nature engagement is emerging as a promising way to support wellbeing for individuals living with long-term conditions.
As interest grows in holistic, person-centred approaches to rehabilitation, nature engagement is emerging as a promising way to support wellbeing for individuals living with long-term conditions.
Nature engagement is endless and broad, and it can range from a forest walk, gardening, horticultural engagement, horse riding and many more possibilities!
Research suggests that spending time in natural environments can offer meaningful benefits such as improvements in mood, confidence, social connection, and overall quality of life for people with neurological conditions. Many people describe nature as a space where they feel more motivated, more independent and more able to challenge themselves in their rehabilitation journey.
To date, despite all these findings, there remains limited research exploring the personal experiences of nature engagement for people with neurological conditions.
Izzy and Rocksy want to contribute to stroke survivors – they state that ‘understanding these perspectives is essential for developing accessible, effective and meaningful nature-based programmes that actually reflect what stroke survivors value and need’.
This study aims to gather the experiences of people who have experienced stroke and who take part in any form of nature-based activity.
The Southampton students would like to understand better, things like:
- What nature means to you?
- What helps or prevents you to engage with it?
- How does it support or challenge your wellbeing and daily life?
 Your insights can help shape future stroke rehabilitation approaches and ensure that nature-based programmes are designed with lived experience at their core.
Your insights can help shape future stroke rehabilitation approaches and ensure that nature-based programmes are designed with lived experience at their core.
Your insights will help us understand what makes it easier or harder to take part in these kinds of activities and how they can be made more accessible for everyone.
 What will happen to me if I take part?
What will happen to me if I take part?
- If you agree to take part, we will ask you to fill in a consent form and a short form to provide background information about you.
- You will be invited to a one-to-one interview lasting around 45–60 minutes. This will take place online via Microsoft Teams at a time that suits you.
- During the interview, we will ask you about your experiences with nature-based activities, the factors that make participation easier or harder, and what you feel the benefits are.
- The interview will be video recorded on Microsoft teams (with your consent) to help us accurately transcribe what is said. The recording will be securely deleted once the transcription is complete. We will remove any identifying information about you from the transcript.
- This transcript will be securely stored on a University of Southampton SharePoint site, accessible to the research team. You do not need to answer any questions that make you feel uncomfortable. You can take breaks or stop the interview at any time..
 Are there any benefits in my taking part?
Are there any benefits in my taking part?
Yes! Your views will contribute to raising awareness and improving understanding of how nature-based interventions are experienced and delivered.
The Southampton students hope that your participation will help inform future practice and promote greater inclusivity for people living with long term neurological conditions. Please contact them on either im2g23@soton.ac.uk or ra11g23@soton.ac.uk
The findings from this study will also be used to teach undergraduate students about the value and application of nature based programmes.
The aim is to gain insight into barriers and enablers that impact engagement in nature-based programmes, and to understand how these activities can be improved and sustained to better support the wellbeing of people with long-term neurological conditions.
The project is not funded in any way.
* Researchers: Izzy Mason, Undergraduate Researcher (BSc Occupational Therapy) University of Southampton and Rocksy Antonygnaneswaran, Undergraduate Researcher (BSc Occupational Therapy), University of Southampton.
* Supervisor: Long-time friend of ARNI Stroke Rehab UK Charity: Dr Leisle Ezekiel (lezekiel@soton.ac.uk)
Dong, Y., Tang, L., Salwismawati Badrin, Salziyan Badrin and Wu, J. (2025). Factors associated with post-stroke fatigue among stroke survivors: a cross-sectional study. PeerJ, 13, pp.e19052–e19052.

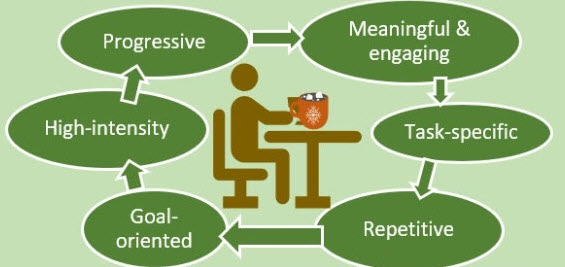 Upper limb impairment is a common and persistent consequence of stroke, significantly affecting an individual’s independence and quality of life. The evidence shows clearly that the cornerstone of effective motor recovery is task-specific practice, a principle underpinned by evidence from neuroscience and motor learning theory. This approach posits that the brain re-organises itself in response to intensive and repetitive functional training, fostering neuroplasticity.
Upper limb impairment is a common and persistent consequence of stroke, significantly affecting an individual’s independence and quality of life. The evidence shows clearly that the cornerstone of effective motor recovery is task-specific practice, a principle underpinned by evidence from neuroscience and motor learning theory. This approach posits that the brain re-organises itself in response to intensive and repetitive functional training, fostering neuroplasticity. This approach moves beyond general exercises to focus directly on the functional skills that enhance independence, motivating patients through visible, goal-oriented progress. While private clinics can offer the benefit of therapist supervision, specialised equipment and intensive regimens, stroke survivors reading this will be all too aware that consistent practice at home is crucial for achieving high dosages of repetition rates necessary for effective motor learning. ARNI Stroke Rehab UK instructors work with patients to set up personalised routines, often leveraging accessible technology or adapted household items, making rehabilitation a continuous, integrated part of daily life.
This approach moves beyond general exercises to focus directly on the functional skills that enhance independence, motivating patients through visible, goal-oriented progress. While private clinics can offer the benefit of therapist supervision, specialised equipment and intensive regimens, stroke survivors reading this will be all too aware that consistent practice at home is crucial for achieving high dosages of repetition rates necessary for effective motor learning. ARNI Stroke Rehab UK instructors work with patients to set up personalised routines, often leveraging accessible technology or adapted household items, making rehabilitation a continuous, integrated part of daily life. For task-specific practice to be effective, it should be relevant to the survivor’s goals, performed frequently, and incorporate feedback to reinforce learning. However, traditional-type therapy has been evidenced to struggle to provide the sheer volume of high-quality repetitions needed to drive meaningful neural recovery. Correspondingly, a range of technologies have emerged fill this need to assist and optimise task-specific practice.
For task-specific practice to be effective, it should be relevant to the survivor’s goals, performed frequently, and incorporate feedback to reinforce learning. However, traditional-type therapy has been evidenced to struggle to provide the sheer volume of high-quality repetitions needed to drive meaningful neural recovery. Correspondingly, a range of technologies have emerged fill this need to assist and optimise task-specific practice. Clinics can now days employ some very sophisticated robotic and electromechanical systems to maximise task-specific training, with many devices in the range of the average stroke survivor’s pocket. Some of these devices are robotic exoskeletons that provide adjustable arm weight support, allowing individuals with severe weakness to perform a greater range of movement. The principle of gravity compensation enables survivors to initiate and control movements themselves, rather than being passively moved, which is crucial for neuroplasticity.
Clinics can now days employ some very sophisticated robotic and electromechanical systems to maximise task-specific training, with many devices in the range of the average stroke survivor’s pocket. Some of these devices are robotic exoskeletons that provide adjustable arm weight support, allowing individuals with severe weakness to perform a greater range of movement. The principle of gravity compensation enables survivors to initiate and control movements themselves, rather than being passively moved, which is crucial for neuroplasticity. For instance the Hocoma ArmeoSpring Pro (right) is a robotic exoskeleton system which provides adjustable arm weight support for the entire movement chain, from the shoulder to the hand, through a patented technology. This counterbalances gravity, allowing individuals with severe weakness to perform a greater range of movement.
For instance the Hocoma ArmeoSpring Pro (right) is a robotic exoskeleton system which provides adjustable arm weight support for the entire movement chain, from the shoulder to the hand, through a patented technology. This counterbalances gravity, allowing individuals with severe weakness to perform a greater range of movement. For instance, the Neofect Smart Glove (left), is a soft, wearable hand-and-wrist rehabilitation device that uses gamified exercises to improve motor function which incorporates sensors that track movements of the wrist and fingers, providing a platform for therapy with accompanying software offering a variety of games targeting different movements and abilities…
For instance, the Neofect Smart Glove (left), is a soft, wearable hand-and-wrist rehabilitation device that uses gamified exercises to improve motor function which incorporates sensors that track movements of the wrist and fingers, providing a platform for therapy with accompanying software offering a variety of games targeting different movements and abilities…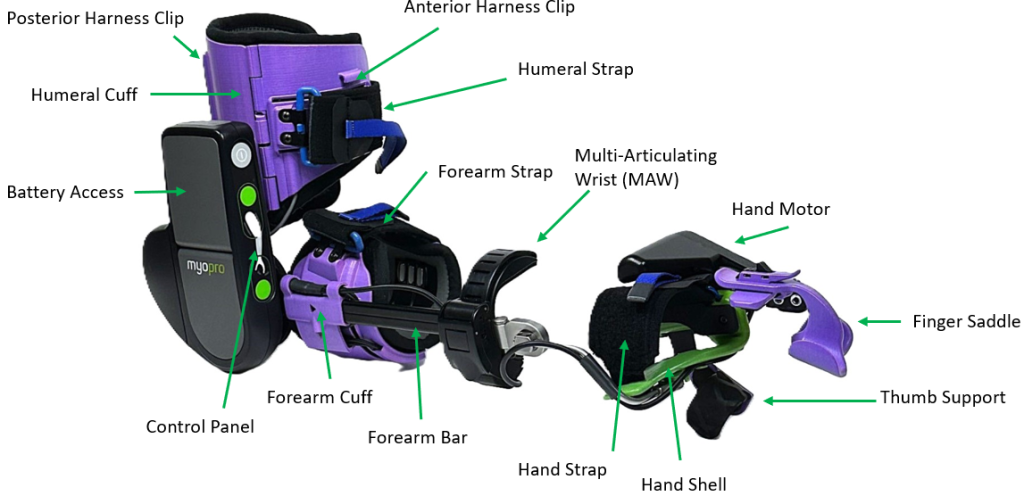 The principle here is to leverage a survivor’s own bio-signals to drive movement, creating a powerful biofeedback loop that promotes active participation and self-initiation of movement.
The principle here is to leverage a survivor’s own bio-signals to drive movement, creating a powerful biofeedback loop that promotes active participation and self-initiation of movement.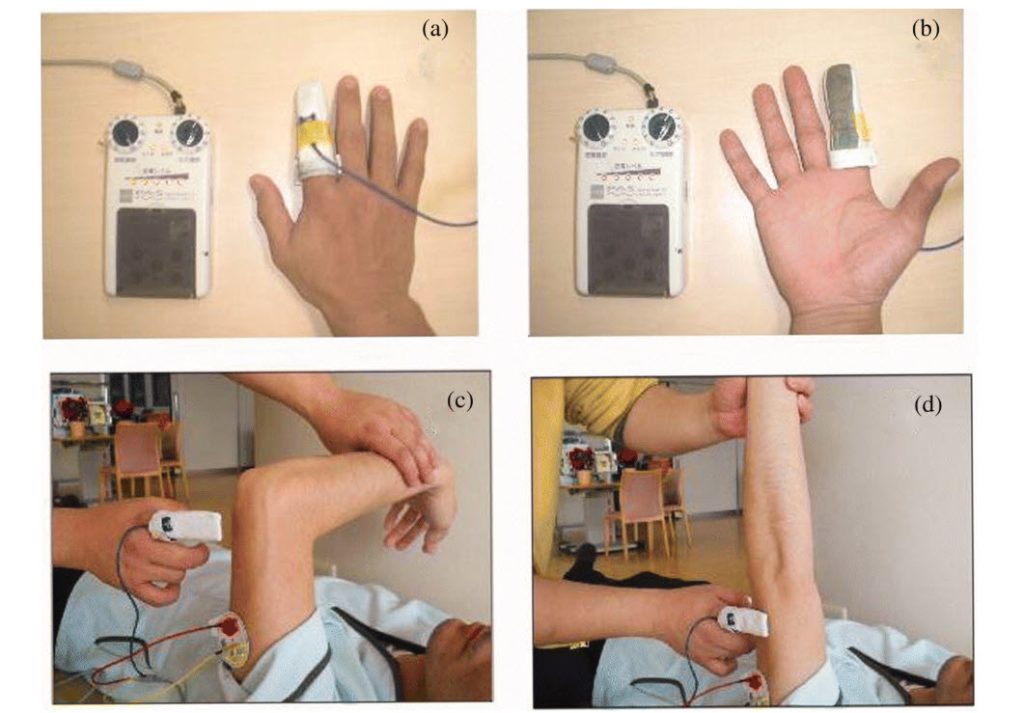 The principle is to provide an external impetus for muscle contraction, which, when paired with the stroke survivor’s intent during a functional task, strengthens the neural pathways controlling movement. This helps re-educate the neuromuscular system and can enable the ability to perform task-specific practice. Clinical access to such FES systems is available through NHS and private rehabilitation services, with pricing depending on the clinical package.
The principle is to provide an external impetus for muscle contraction, which, when paired with the stroke survivor’s intent during a functional task, strengthens the neural pathways controlling movement. This helps re-educate the neuromuscular system and can enable the ability to perform task-specific practice. Clinical access to such FES systems is available through NHS and private rehabilitation services, with pricing depending on the clinical package.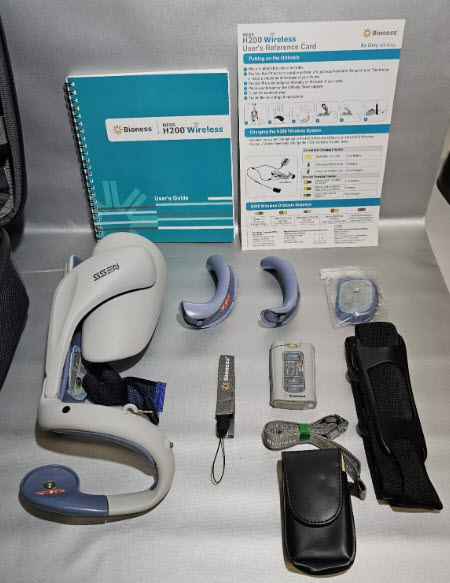 An example of a wearable for the home market is the Bioness H200 Wireless; (right) a sleek, wireless FES device that delivers mild electrical stimulation to specific arm and hand muscles via electrodes integrated into a soft cuff. The stimulation is controlled via an intuitive handheld unit or app, allowing for functional, task-specific training. The core principle is that FES provides an external impetus for muscle contraction, which, when paired with the patient’s intent to move, strengthens the neural pathways controlling arm and hand function.
An example of a wearable for the home market is the Bioness H200 Wireless; (right) a sleek, wireless FES device that delivers mild electrical stimulation to specific arm and hand muscles via electrodes integrated into a soft cuff. The stimulation is controlled via an intuitive handheld unit or app, allowing for functional, task-specific training. The core principle is that FES provides an external impetus for muscle contraction, which, when paired with the patient’s intent to move, strengthens the neural pathways controlling arm and hand function.  Others incorporating FES and EMG which are designed for survivors to purchase, like the
Others incorporating FES and EMG which are designed for survivors to purchase, like the 
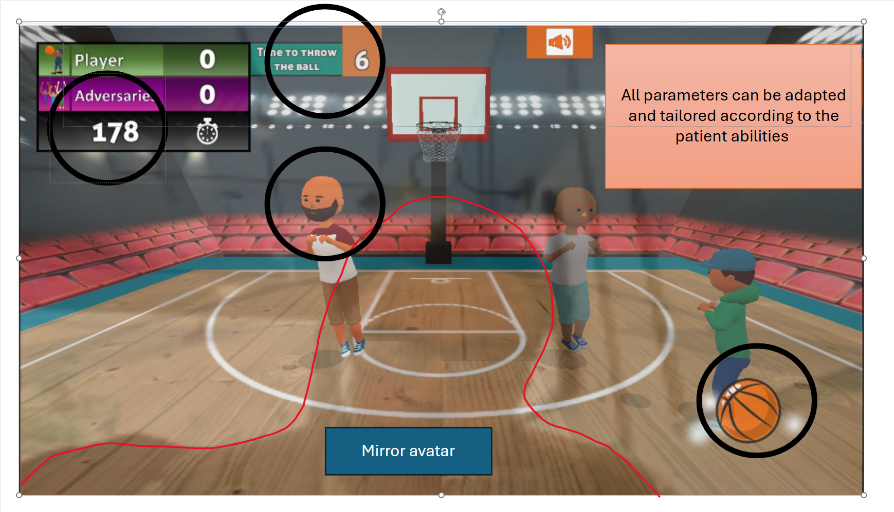
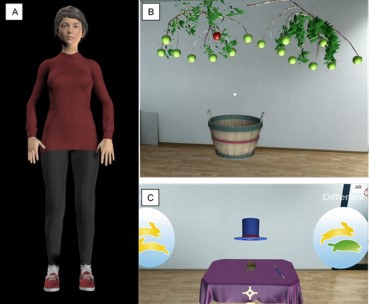
 Virtual Reality (VR) is transforming monotonous exercises into interactive games, boosting patient engagement and motivation. Studies have shown that when used alongside traditional therapy, VR can significantly improve motor function and quality of life for stroke survivors.
Virtual Reality (VR) is transforming monotonous exercises into interactive games, boosting patient engagement and motivation. Studies have shown that when used alongside traditional therapy, VR can significantly improve motor function and quality of life for stroke survivors. Robotic devices can also supplement therapy by assisting with intensive, repetitive exercises that might otherwise be too demanding for therapists or patients. The best results often occur when robotic therapy is combined with conventional methods, and different robots are suited for varying needs.
Robotic devices can also supplement therapy by assisting with intensive, repetitive exercises that might otherwise be too demanding for therapists or patients. The best results often occur when robotic therapy is combined with conventional methods, and different robots are suited for varying needs.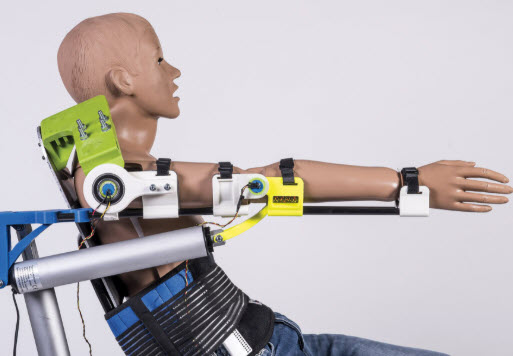 Upper limb exoskeletons operate in several modes to help with different stages of recovery:
Upper limb exoskeletons operate in several modes to help with different stages of recovery: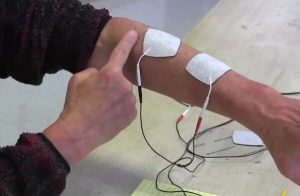 Functional Electrical Stimulation (FES) uses electrical pulses to activate muscles artificially, helping to practice functional tasks like grasping and reaching. When coupled with voluntary movement, this technique can help promote neuroplasticity, the brain’s ability to reorganize itself. Surface electrodes can be placed on the skin, or in more advanced setups, integrated into electrode arrays on a fabric sleeve or orthosis.
Functional Electrical Stimulation (FES) uses electrical pulses to activate muscles artificially, helping to practice functional tasks like grasping and reaching. When coupled with voluntary movement, this technique can help promote neuroplasticity, the brain’s ability to reorganize itself. Surface electrodes can be placed on the skin, or in more advanced setups, integrated into electrode arrays on a fabric sleeve or orthosis. Wearable sensors take the form of wrist-worn sensors or special gloves can track arm movements and provide real-time feedback through a tablet or app. Gamified devices have also been available for many years. Both the following are produced by long-term colleagues of ARNI: GripAble, is a great example which turns exercises into engaging, fun activities for at-home use. And Neuroball
Wearable sensors take the form of wrist-worn sensors or special gloves can track arm movements and provide real-time feedback through a tablet or app. Gamified devices have also been available for many years. Both the following are produced by long-term colleagues of ARNI: GripAble, is a great example which turns exercises into engaging, fun activities for at-home use. And Neuroball


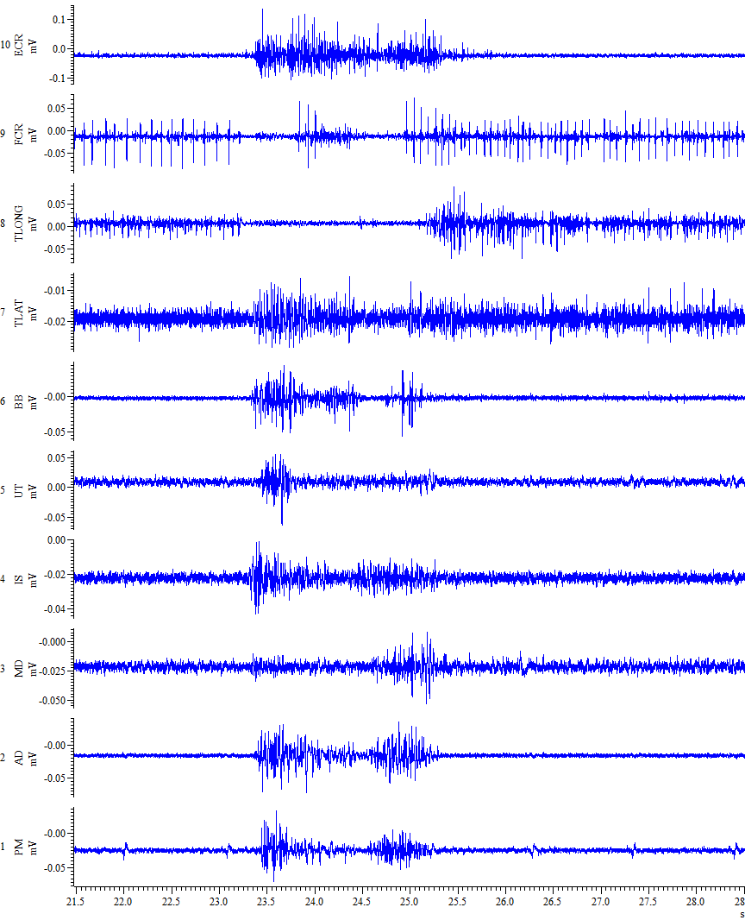 This study is proof of concept that aims to see whether even short-term use of such a game can make a measurable difference. And now, they are inviting participants to get involved too.
This study is proof of concept that aims to see whether even short-term use of such a game can make a measurable difference. And now, they are inviting participants to get involved too.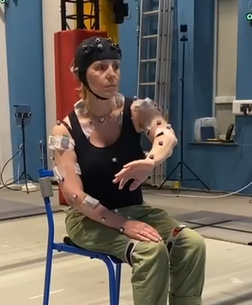 You’ll attend a session at the VSimulators facility in Exeter or University of Leeds. The session takes about 2 hours, including preparation and testing.
You’ll attend a session at the VSimulators facility in Exeter or University of Leeds. The session takes about 2 hours, including preparation and testing.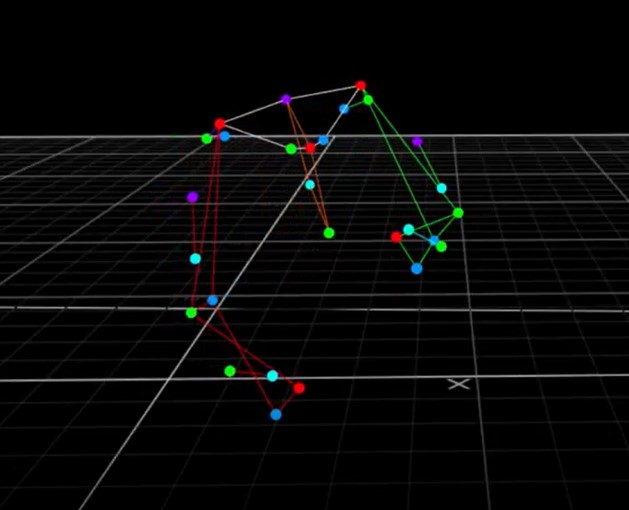
 Your GP no doubt has already told you that if he or she could put cardiovascular exercise into a drug, it would be one of the most effective medications to prevent and/or treat patients with cardiovascular and/or cerebrovascular diseases. But cardiovascular exercise, despite the known benefits, is still known to be under-utilised by clinicians as a ‘prescription’ during rehabilitation.
Your GP no doubt has already told you that if he or she could put cardiovascular exercise into a drug, it would be one of the most effective medications to prevent and/or treat patients with cardiovascular and/or cerebrovascular diseases. But cardiovascular exercise, despite the known benefits, is still known to be under-utilised by clinicians as a ‘prescription’ during rehabilitation.

 The evidence for exercise after stroke has resulted in the development of stroke-specific community exercise programmes. The system is analogous to the very well-established rehabilitation services for cardiac disease patients which usually start after usual rehabilitation has ended. Collaborations between health boards and council-run leisure centres have resulted in the establishment of exercise referral schemes, which have provided a range of stroke-specific cardiovascular exercise programmes delivered to smaller and larger groups.
The evidence for exercise after stroke has resulted in the development of stroke-specific community exercise programmes. The system is analogous to the very well-established rehabilitation services for cardiac disease patients which usually start after usual rehabilitation has ended. Collaborations between health boards and council-run leisure centres have resulted in the establishment of exercise referral schemes, which have provided a range of stroke-specific cardiovascular exercise programmes delivered to smaller and larger groups. Those that are known as recumbent or semi-recumbent bikes (depending how reclined it is) would be my first choice for a ‘beginner stroke survivor’. These types of gym bikes can be picked up relatively affordably from a variety of places and often aren’t cheap but they hold a considerable re-sale value.
Those that are known as recumbent or semi-recumbent bikes (depending how reclined it is) would be my first choice for a ‘beginner stroke survivor’. These types of gym bikes can be picked up relatively affordably from a variety of places and often aren’t cheap but they hold a considerable re-sale value.
 A big tip from Tom: make sure to record and celebrate any and all successes. Try to pinpoint how you achieved new action control in your ADLs. This is often via something achieved in your retraining. Start to become aware of these. Get this data recorded somehow.
A big tip from Tom: make sure to record and celebrate any and all successes. Try to pinpoint how you achieved new action control in your ADLs. This is often via something achieved in your retraining. Start to become aware of these. Get this data recorded somehow.

 Also, note as an aside that if ‘Press’ may involve ‘where one creates’ / where/who is around to help you do stuff / what sources can you look at / involve with etc etc, it does rather shine a light on the importance of being cognisant of not just ‘where one is’ (eg, in a flat, in a tower block, in the suburbs of London) but how one can bring maximal resources to bear to help your own situation.
Also, note as an aside that if ‘Press’ may involve ‘where one creates’ / where/who is around to help you do stuff / what sources can you look at / involve with etc etc, it does rather shine a light on the importance of being cognisant of not just ‘where one is’ (eg, in a flat, in a tower block, in the suburbs of London) but how one can bring maximal resources to bear to help your own situation.
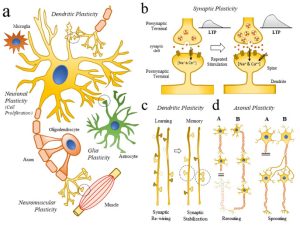 Your brain attempts to repair as much as possible after stroke, but there is a downside. During this period of repair, the neurons that surround the infarct are not able to do their job of conducting impulses.
Your brain attempts to repair as much as possible after stroke, but there is a downside. During this period of repair, the neurons that surround the infarct are not able to do their job of conducting impulses. The more a road is used or the more popular it may become (ie, if a new short-cut to a motorway has just been loaded to the sat-nav technology), the more traffic may build suddenly up along that route, so the council may strengthen the existing road to cope with the traffic and/or add more lanes or new routes to cope with the increased traffic (new connections). It will also add speed-bumps no doubt!
The more a road is used or the more popular it may become (ie, if a new short-cut to a motorway has just been loaded to the sat-nav technology), the more traffic may build suddenly up along that route, so the council may strengthen the existing road to cope with the traffic and/or add more lanes or new routes to cope with the increased traffic (new connections). It will also add speed-bumps no doubt! Neuroplasticity allows us to compensate for irreparably damaged neural pathways by strengthening or re-routing remaining ones. The more you use these pathways, your brain will respond by upgrading them so that they’re more efficient at handling the traffic and the quicker the information is sent. The more the pathways (or ‘roads’) are used, the more adequately functional a task, ability or skill may seem to become.
Neuroplasticity allows us to compensate for irreparably damaged neural pathways by strengthening or re-routing remaining ones. The more you use these pathways, your brain will respond by upgrading them so that they’re more efficient at handling the traffic and the quicker the information is sent. The more the pathways (or ‘roads’) are used, the more adequately functional a task, ability or skill may seem to become. A big secret to success with your upper limb for example (dependent on presentation) is, after early intensive recovery efforts have moved you to a certain standard of functional movement, to start ‘creating’ things with the thought of ‘formal rehab’ firmly in the background.
A big secret to success with your upper limb for example (dependent on presentation) is, after early intensive recovery efforts have moved you to a certain standard of functional movement, to start ‘creating’ things with the thought of ‘formal rehab’ firmly in the background. And furthermore, motivation must ‘run like a ribbon’ through the creative process. This must be intrinsic to the creator – there must be a NEED to create, to problem-solve until an objective is complete. This need stokes interest, drive, enthusiasm, desire, perseverance, passion and persistence.
And furthermore, motivation must ‘run like a ribbon’ through the creative process. This must be intrinsic to the creator – there must be a NEED to create, to problem-solve until an objective is complete. This need stokes interest, drive, enthusiasm, desire, perseverance, passion and persistence.
 Dr Tom Balchin, who founded the Action for Rehabilitation from Neurological Injury (ARNI) Charity nearly 25 years ago, has been made an Officer of the British Empire (OBE) in the New Year’s Honours List.
Dr Tom Balchin, who founded the Action for Rehabilitation from Neurological Injury (ARNI) Charity nearly 25 years ago, has been made an Officer of the British Empire (OBE) in the New Year’s Honours List.  To do this required Dr Tom create what has become the only existing national accredited qualification in rehabilitation after stroke for specialist personal trainers and therapists.
To do this required Dr Tom create what has become the only existing national accredited qualification in rehabilitation after stroke for specialist personal trainers and therapists.


 Sheffield Teaching Hospitals and NHS Trusts nationally are looking for stroke survivors (aged 18+) with persistent arm weakness following an ischaemic stroke, which occurred between 6 months and 10 years ago.
Sheffield Teaching Hospitals and NHS Trusts nationally are looking for stroke survivors (aged 18+) with persistent arm weakness following an ischaemic stroke, which occurred between 6 months and 10 years ago. 





 Are between 40-80 years of age.
Are between 40-80 years of age.
 ANDREW (BY MARION). September 2024.
ANDREW (BY MARION). September 2024.