
Not a News Item today, but an important Technical Reminder: for our stroke survivors and their professional therapists and ARNI neuro-instructors, navigating the complexities of recovery, understanding the mechanics of symptoms is critical. One of the questions that these groups ask experts in stroke is exactly why spasticity is negatively affected by movement speed.
So, one of the most defining characteristics of spasticity after stroke is its reliance on velocity – in effect, the question isn’t just if there is resistance, but how quickly you move. This phenomenon is rooted entirely in the intricate neurophysiology of the spinal cord reflex arc and the disruption caused by an upper motor neuron (UMN) lesion.
In a healthy system, our muscle tone is finely tuned by a balance of excitatory and inhibitory signals. After a UMN lesion, perhaps from a stroke or spinal cord injury, this descending inhibitory control is diminished or lost. The spinal circuitry becomes disinhibited, hypersensitive to input. The key sensory players here are the muscle spindles; specialised receptors within the muscle belly that detect changes in length and the speed of those changes.
The primary afferent fibers (Group Ia afferents) innervating these spindles are exquisitely sensitive to the velocity of a stretch. When a therapist or trainer moves a limb which is in in a position of spasticity, stretching the muscle, these velocity-sensitive fibers fire robustly. The faster the movement, the greater the electrical signal transmitted back to the spinal cord. In the disinhibited state, this heightened afferent barrage leads to an exaggerated excitation of the alpha motor neurons, the final common pathway for muscle contraction.
The result is an abnormally strong, brisk, exaggerated involuntary efferent contraction, which manifests clinically as increased resistance proportional to the speed of the stretch applied. This mechanism distinguishes spasticity from other forms of hypertonia like rigidity, which is velocity-independent. Understanding this principle is crucial for effective therapy; it’s why slow, sustained stretches are often more effective than quick movements in managing spasticity and why careful grading of speed is vital during functional tasks…
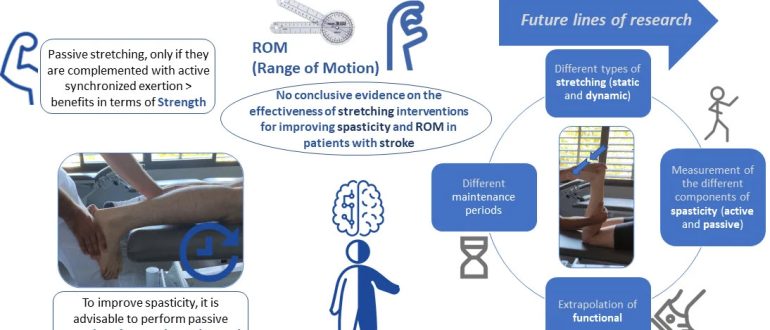
So, essentially, speed is the key trigger! The quicker the movement, the stronger the sensory feedback that bypasses normal modulation, resulting in that characteristic resistance we measure clinically, using scales like the Modified Ashworth Scale (MAS) and the Tardieu Scale (evaluating stretch reflex at different speeds).
For more about spasticity, please see this post on the ARNI site from 2019: https://arni.uk.com/spasticity-after-stroke-will-my-hand…/
