An update of ‘where we are’ as far as stem cell therapy for stroke survivors is concerned. So, stem cell therapy is, as you probably know very well, not currently recommended as a standard treatment for ischemic stroke patients due to insufficient evidence of clinical efficacy, despite promising preclinical results.
Despite the limitations of current standard treatments, stem cell therapy remains investigational. No mention of stem cell therapy appears in any of the major stroke treatment guidelines.
Multiple stem cell types have been investigated in preclinical and clinical studies:
- Mesenchymal stem cells
- Neural stem cells
- Bone marrow mononuclear cells
- Embryonic stem cells
- Induced pluripotent stem cell-derived neural stem cells
Proposed mechanisms of action include:
- Cell differentiation and replacement
- Immunomodulation
- Neural circuit reconstruction
- Release of protective factors
The most recent and highest quality evidence comes from a 2021 systematic review and meta-analysis of randomized controlled trials. An analysis of 8 RCTs involving 459 subjects (217 intervention, 242 controls) shows:
- No significant reduction in neurological deficit (NIHSS score) in acute or subacute stroke
- Some benefit observed in chronic stroke patients, but clinical significance unclear
- No statistically significant reduction in mortality rates
Overall conclusion: No clinically important evidence for efficacy of stem cells in reducing neurological deficit compared to control group.
Challenges and Limitations
Several issues remain unresolved regarding stem cell therapy for stroke:
- Cell type selection
- Dosing regimens
- Delivery routes (IV vs. intra-arterial)
- Timing of administration
- Translation challenges from bench to bedside:
- Conflicting results between preclinical and clinical studies
- Mechanisms of action not fully understood
- Limited therapeutic window in most clinical trials
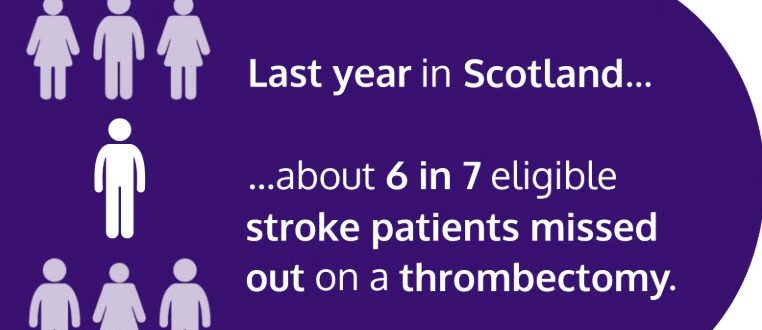
So, patients reading the ARNI News page who are interested in stem cell therapy should be referred to centers conducting approved clinical trials, avoiding unproven commercial stem cell treatments outside of regulated research settings. While stem cell therapy shows theoretical promise for ischemic stroke treatment, current evidence does not support its use in routine clinical practice. Established treatments like thrombolysis and endovascular therapy remain the standard of care for improving outcomes in ischemic stroke patients.