

 So many stroke survivors, at varying points during their respective times from stroke, have no idea how to start (or re-start) their recoveries. Or they do know about some options. But in either circumstance a majority don’t know what to do for themselves to stand the best chances of gaining some functional success for their efforts.
So many stroke survivors, at varying points during their respective times from stroke, have no idea how to start (or re-start) their recoveries. Or they do know about some options. But in either circumstance a majority don’t know what to do for themselves to stand the best chances of gaining some functional success for their efforts.
This blog could help you get over both hurdles. Read and enjoy!
First, most stroke survivors can be assisted by advising them to have one ‘go-to’ safe and accessible place to regularly train (eg. a small matted ‘training area’, which needs only to be a few square metres wide, plus a small table and a chair), how to accumulate bits of kit (adjuncts to optimise re-training), depending on needs and budget, and a set amount of times per week in which to devote to retraining as well as how to perform much more regular (often upper-limb) functional re-training and maybe ‘what with’.
This is a all a great start, and most often needs help to do from physio or trainer qualified in stroke rehab.
Here’s how you can view re-training (my combo of rehab and training!): functional re-training isn’t just about attempting to do more and more difficult things around the house and outside. It is a specific re-training regimen combined with the everyday checking of progress.
For instance, upper-limb ADL progress checking would mean making trying out upper limb tasks in your environment, evaluating your status on each (if you can). So, if on one day you tried to open windows or doors and switch on the kettle or lights around the house, and on another day, you attempted to load a cutlery drawer and use a keyboard or remote control, you need to note in a diary or into an app if you have a perceived success in aspects of those activities where you had none or little before.
This may allow you to see if you can relate progressions to anything specific you may have been working on in retraining. It’s possible to become really ‘switched on’ to the smallest of progressions by doing this, which of course keeps retraining stimulating and ‘worth doing’.
Specific task-training can be very taxing to do however, if you have barely got the underlying motor control to initiate a movement. Read below what you can do, instead, at home if you don’t. It was one of the keys to my own success when recovering from a serious stroke, which I had to work out for myself at the time.
My tip for you is that by continually noting what seems to you to be progressions in ability (even if you’re ‘wrong’ in the view of a physio or trainer if you happen to have one) is a great way to give yourself constant boosts and keep motivated.
Keep self-evaluating. Functional retraining works well if you can create this kind of continual feedback loop to inform your next sessions and general optimistic outlook (if you can, of course). And this kind of charting/noting ‘what has been done/achieved’ is a good way also to begin to tackle fatigue, if you have it, over time.
To attempt doing this, you also need if you can to try your hardest to be ‘well-informed’ about the nature of stroke and the extent to which it really is possible to get back useful function after stroke in order that you’re not fooling yourself in terms of progression.
 The reason why it’s important to be able to ‘contextualise/frame yourself’ in terms of the possible progress you can make by comparing yourself to existing data (seeing where you might fit or be one of those outliers etc), is that in the community, it’s very unlikely that you’ll be able to have any of the types of measures applied to you that therapists use clinically on patients unless one is working actively with a therapist.
The reason why it’s important to be able to ‘contextualise/frame yourself’ in terms of the possible progress you can make by comparing yourself to existing data (seeing where you might fit or be one of those outliers etc), is that in the community, it’s very unlikely that you’ll be able to have any of the types of measures applied to you that therapists use clinically on patients unless one is working actively with a therapist.
We do, at ARNI, regular assessments with patients including Stroke Impact Scale, CAHAI (and arm and hand function measure) and a few others, but in the community in general, especially if just attending a group class, it’s quite rare to be have any kind of ‘assessment of training or quality of life progress’.
So the key to this all is to remember that tasks performed in retraining to help you perform ADLs don’t just have to definitely be the tasks themselves (for practical reasons). They can also be trained for via ‘close-simulations’.
These rely on you finding your own task specifics, according to your goals, and finding ways to work on them in a training area and then phasing to do/practice them outside the training area. Something as ‘everyday’, pre-stroke, as grasping and pushing a shopping trolley may have to be worked on intensively after stroke. And a therapist or trainer can help you to access these things by setting up situations to introduce concepts to you and ways to practice (do as many reps as possible and in the most appropriate way(s) possible.
 For instance, if you love playing golf and really want to get back to it after stroke, it might not be appropriate to practise straightaway with your Number 5 iron in your house, unless you have a high ceiling and your control is already very good!
For instance, if you love playing golf and really want to get back to it after stroke, it might not be appropriate to practise straightaway with your Number 5 iron in your house, unless you have a high ceiling and your control is already very good!
But by getting someone to cut a broom handle in half and chamfering each end for you, you have a tool which can help you to practise your hand placement on the club and your swing without problems until you can start to use a real one again.
You can see also that this idea would help negate the leverage weight of a real golf club.
I show my trainers how to use some tape to bind a short, weighted stick to a survivor’s hand, which allows the survivor to rotate it back and forth to build wrist-strength without it falling from his grip. Weighted sticks can be made by taping tiny weights to the stick. This work can really help the survivor position the hand for grasp-type tasks.
Lots more ideas like that can be found here www.successfulstrokesurvivor.com including how to make (or get someone to make for you), a method to practice using a steering wheel.
There are other ways that you can practice for getting back to some of the pursuits you liked pre-stroke. VR works well here. People who want to be pilots take advantage of simulated work throughout their years of learning. Stroke survivors, like pilots, can get closer and closer to the real thing via this immersive learning tactic. So here, the survivor could try and go to an indoor golf simulator centre.
Even though simulations are not posited to be quite as efficient for motor learning as performing the real thing, working like this keeps you in the training area, keeps you working on-task, allows for gradated practise and keeps you safe. And then crucially, outside of the training area, you need to try to practice the tasks (or the components of them that you can manage) repetitively, as part of your ADLs. And evaluating.
So, to sum:
- You need to practice the real task itself, if possible, in your training area.
- If the real task isn’t able to be done with your current limitations or isn’t appropriate to perform in your training area, practice using as close simulations in your training area as possible.
- Progress on the real task must consistently be checked outside your training area.
Much more about all this in the Successful Stroke Survivor manual/handbook – very recently updated/printed copies available only from www.successfulstrokesurvivor.com
PLEASE SHARE THIS BLOG POST OVER TO ANYONE WHOM YOU MIGHT THINK COULD BENEFIT! MANY THANKS TO YOU…


 Finding a Speech and Language therapist after discharge is notoriously difficult and SLTs are almost exclusively clinical and/or have big case-loads to take care of. And we know that SLT is often prohibitively expensive to engage with or just unaffordable, meaning people just get incredibly frustrated.
Finding a Speech and Language therapist after discharge is notoriously difficult and SLTs are almost exclusively clinical and/or have big case-loads to take care of. And we know that SLT is often prohibitively expensive to engage with or just unaffordable, meaning people just get incredibly frustrated.
 Storm Anderson, a UK-based speech and language therapist who has predominately treated adults affected by stroke and other acquired brain injury in acute hospital settings as well as out-patient and home-based settings. She has completed her BSc in Speech Language Pathology and MSc in Stroke Medicine, and is currently undertaking her PhD at Queen Square, UCL, using the PLORAS (Predicting Language Outcomes After Stroke) datasets.
Storm Anderson, a UK-based speech and language therapist who has predominately treated adults affected by stroke and other acquired brain injury in acute hospital settings as well as out-patient and home-based settings. She has completed her BSc in Speech Language Pathology and MSc in Stroke Medicine, and is currently undertaking her PhD at Queen Square, UCL, using the PLORAS (Predicting Language Outcomes After Stroke) datasets. Olivia Hodgkinson, a Johannesburg-based qualified Speech Language therapist who completed her BSc and MSc in Speech and Language Pathology at Cape Town University. She has substantial experience in both clinical (acute, sub-acute, specialised rehab and extended units) and educational settings. who has worked within highly diverse settings and within multidisciplinary teams and units. She has led and run therapy departments, supervised and mentored speech therapy university students, developed school based educational assessment programs and support structures for specialised learning units, initiated and implemented training for staff, allied professionals, family and caregivers on a variety of scope related topics in school, hospital and community based settings. She has strong dysphagia experience and skills and is a certified Vital-stim practitioner. She has a great passion for adult neurological injuries and disorders, voice disorders and dysphagia and is looking forward to helping you!
Olivia Hodgkinson, a Johannesburg-based qualified Speech Language therapist who completed her BSc and MSc in Speech and Language Pathology at Cape Town University. She has substantial experience in both clinical (acute, sub-acute, specialised rehab and extended units) and educational settings. who has worked within highly diverse settings and within multidisciplinary teams and units. She has led and run therapy departments, supervised and mentored speech therapy university students, developed school based educational assessment programs and support structures for specialised learning units, initiated and implemented training for staff, allied professionals, family and caregivers on a variety of scope related topics in school, hospital and community based settings. She has strong dysphagia experience and skills and is a certified Vital-stim practitioner. She has a great passion for adult neurological injuries and disorders, voice disorders and dysphagia and is looking forward to helping you!
 Are you a stroke survivor aged 65 years old or older, who has had a stroke at least 6 months ago?
Are you a stroke survivor aged 65 years old or older, who has had a stroke at least 6 months ago?




 Up to 70% of survivors experience fatigue that includes overwhelming physical and/or mental tiredness or exhaustion. And 50% find tiredness to be their main problem.
Up to 70% of survivors experience fatigue that includes overwhelming physical and/or mental tiredness or exhaustion. And 50% find tiredness to be their main problem. 
 The University of Southampton has started running a research study which builds on previous work where a smartphone app was developed to capture fatigue via a Fit-Bit watch as it happens in real-time.
The University of Southampton has started running a research study which builds on previous work where a smartphone app was developed to capture fatigue via a Fit-Bit watch as it happens in real-time. The aims of this are to:
The aims of this are to:






 Balance perturbation and lower body strength training (again with a therapist or trainer guiding and guarding you to extend your capabilities) are identified as successful further training regimens.
Balance perturbation and lower body strength training (again with a therapist or trainer guiding and guarding you to extend your capabilities) are identified as successful further training regimens.

 Other examples you can explore in
Other examples you can explore in 
 When people have strokes, loss of strength as a result can be extensive and a major contributor to prolonged recovery times. It’s estimated that the strength loss after the stroke is around 50% on the affected side of the body. The reasons for losing strength are related to factors such as weak neural activity after a brain injury and losing muscle mass (atrophy).
When people have strokes, loss of strength as a result can be extensive and a major contributor to prolonged recovery times. It’s estimated that the strength loss after the stroke is around 50% on the affected side of the body. The reasons for losing strength are related to factors such as weak neural activity after a brain injury and losing muscle mass (atrophy).

 For example, by the severity of your difficulties and perceived losses, your individual coping style, your familial/social support network, your cultural beliefs about disability, and your previous mental-health.
For example, by the severity of your difficulties and perceived losses, your individual coping style, your familial/social support network, your cultural beliefs about disability, and your previous mental-health. For example, it may be best to avoid crowds and stressful conditions, which may in turn make you feel overwhelmed. You can try learning relaxation techniques to help you combat any stress and fatigue you may experience after your stroke. There are lots of devices and apps to help you manage to bring emotions to an equilibrium over time.
For example, it may be best to avoid crowds and stressful conditions, which may in turn make you feel overwhelmed. You can try learning relaxation techniques to help you combat any stress and fatigue you may experience after your stroke. There are lots of devices and apps to help you manage to bring emotions to an equilibrium over time.
 Apathy can have negative impact on your recovery of function, your ADLs, general health, and quality of life. It can stop you from enjoying your social connections and bothering to do things that you enjoy. If you develop apathy, it can also lead to a significant extra burden for your families, carers and friends… and worries them because it’s obvious how it will hold you back from potentially conquering/coping better w the situation you’re in.
Apathy can have negative impact on your recovery of function, your ADLs, general health, and quality of life. It can stop you from enjoying your social connections and bothering to do things that you enjoy. If you develop apathy, it can also lead to a significant extra burden for your families, carers and friends… and worries them because it’s obvious how it will hold you back from potentially conquering/coping better w the situation you’re in. It can be easy to think that emotional changes will never improve, but research shows that you may well come to terms with the after-effects of your stroke, which may in turn help responses and mood to become more balanced.
It can be easy to think that emotional changes will never improve, but research shows that you may well come to terms with the after-effects of your stroke, which may in turn help responses and mood to become more balanced. These are most likely to be experienced by those working with families and carers working with survivors with significant cognitive, communication and physical difficulties. Behaviours can range in severity and most usually have a function such as communicating a frustrated or unmet need. Families and carers have to come to understand these behaviours as best as they can.
These are most likely to be experienced by those working with families and carers working with survivors with significant cognitive, communication and physical difficulties. Behaviours can range in severity and most usually have a function such as communicating a frustrated or unmet need. Families and carers have to come to understand these behaviours as best as they can. Consistent and positive support, such as that offered by an excellent therapist/trainer (a qualified ARNI Instructor being just one example) is a great way to start this, as such a person will come in to the home, offering an encouraging example of health and strength for the survivor to hopefully be motivated by, and will know many innovative strategies to trial with the person to help them be creative with their own recoveries.
Consistent and positive support, such as that offered by an excellent therapist/trainer (a qualified ARNI Instructor being just one example) is a great way to start this, as such a person will come in to the home, offering an encouraging example of health and strength for the survivor to hopefully be motivated by, and will know many innovative strategies to trial with the person to help them be creative with their own recoveries.
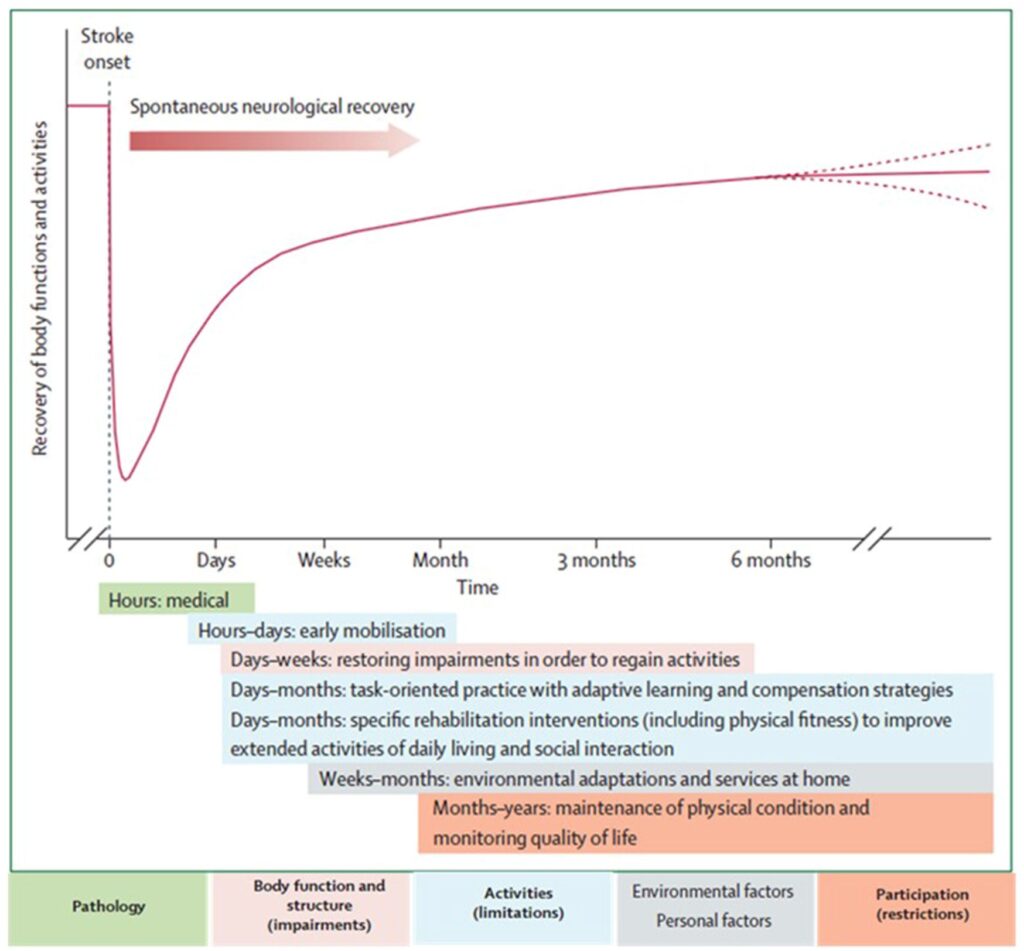 But you must also appreciate that a gradient of significant possible responsiveness to treatment (and also responsiveness to neglect of rehab/retraining) that extends after 12 months post-stroke has been uncovered, which is VERY relevant for the majority of stroke patients.
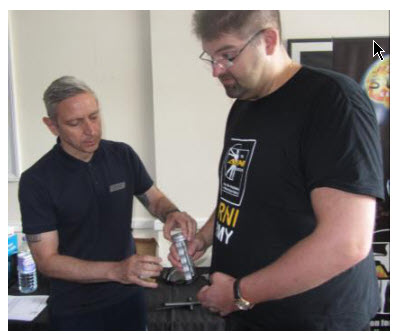
But you must also appreciate that a gradient of significant possible responsiveness to treatment (and also responsiveness to neglect of rehab/retraining) that extends after 12 months post-stroke has been uncovered, which is VERY relevant for the majority of stroke patients. To help with task-training, strength training and developing physical coping (not compensation) strategies, there are also so many adjuncts to community stroke rehab retraining these days – low tech to high tech – from AFO’s that can phase you on from rigid plastic orthotics, to upper limb de-weighting devices, simple and cost-effective devices like the
To help with task-training, strength training and developing physical coping (not compensation) strategies, there are also so many adjuncts to community stroke rehab retraining these days – low tech to high tech – from AFO’s that can phase you on from rigid plastic orthotics, to upper limb de-weighting devices, simple and cost-effective devices like the 




