Welcome to the ARNI Stroke Charity website for stroke survivors, families and healthcare professionals: providing specialist rehabilitation therapy and exercise support after hospital and community physiotherapy finishes.
Please click on the 2025 ARNI Newsletter
Your Stroke / Brain Injury Recovery Starts Here
ARNI home-based training and guidance for your rehab is POWERFUL. Accept no substitute.
Tiredness is something we all experience in our everyday lives. But how about the sort of tiredness which seems to be unrelated to physical or mental exertion, and does not seem to be alleviated by rest? This is a real problem for many stroke survivors on top of the many other problems they may face – and is called ‘fatigue’.
Fatigue is one of the most commonly reported symptoms after Stroke with a prevalence of up to 80%, characterised by overwhelming physical and/or mental tiredness or exhaustion.
For many the symptoms dissipate and lessen over time. Others continue to experience these symptoms at a high level many years after their stroke. This is called chronic fatigue.
Chronic Fatigue has a major impact on Quality of an individual’s life, making everyday tasks feel overwhelming and unachievable, or just plain exhausting. Despite the high prevalence, what causes fatigue to persist for months or years after a stroke remains an open question.
Researchers continue to try and get a better understanding of the mechanisms that underlie fatigue in order to answer this question. Understanding more about it may in turn can maybe lead to the development of effective interventions which may significantly alleviate the condition.
The Effort Lab, led by Dr Anna Kuppuswamy, based at the Institute of Neurology, UCL, in London, has been studying fatigue over the last 10 years to better understand the brain mechanisms that underlie this highly debilitating symptom, not only after Stroke but across other neurological conditions such as Multiple Sclerosis and Parkinson’s Disease.
Their work suggests that altered perception of various sensations can explain the onset and persistence of fatigue.
When performing day to day tasks for example, altered perception will make the tasks feel more effortful. And when in a busy environment with background noise, altered perception results in being overwhelmed and brings on fatigue.
What remains unclear is the relationship between fatigue and visual perception.
They have designed a way that stroke survivors can feedback their experiences to the research team in order to gather important information from various neurological conditions so that they can better understand the possible links.
CALLING ALL STROKE SURVIVORS – PLEASE HELP BY GETTING INVOLVED IN THIS IMPORTANT STUDY IF IT IS APPROPRIATE TO YOUR SITUATION!
It takes no more than 45 minutes on an online combined quiz and questionnaire:
online quiz: completing a couple of questionnaires
online task: identifying shapes and responding by pressing the appropriate buttons on your keyboard.
A tip: For best display of the questionnaire graphics, use a laptop/desktop computer or tablet…
Strong evidence exists that physiotherapy improves the ability of people to move and be independent after suffering a stroke. But at six months after stroke, we know that many people remain unable to produce the movement needed for every-day activities such as answering a telephone. So, what can be done?
1. First, it’s important to be able to recognise if a physiotherapy intervention is really aiding a survivors’ abilities to undertake everyday activities or whether the intervention is doing less than it than it purports to/would ideally do.
This requires a deeper knowledge of the biological underpinnings of neuromuscular function. Neuromuscular function includes the ability to use weak muscles in the right order and at the right time during movement and performing everyday tasks in the same way as you did before the stroke.
2. Second, to optimise a physiotherapist’s chances to advise/work on an optimal combination of rehab interventions for each individual after stroke, it would be ideal to find out what kinds of sleep patterns are most beneficial for them.
Physiotherapists need to be able to have the same opportunity to diagnose how to help each stroke survivor gain the kind of very accurate movement measures at any point in their rehabilitations that currently, only specialist University facilities can routinely produce. This equipment is obviously expensive and can only be used in large specialised laboratories.
Ideally, more portable equipment should also be able to be accessed by therapists, which would cost less and is designed for use in small spaces. But such equipment would have to also be sensitive enough to provide meaningful feedback for therapists in a similar way to those used by the specialist labs. Such feedback could then be very useful for therapists and survivors to create optimal rehab plans together which would really enable the survivor to work on his/her edges of current ability.
A School of Health Sciences research team at the University of East Anglia (UEA) headed up by Professor Valerie Pomeroy have been attempting to find out if this can be done and have also been examining how sleep patterns affect rehabilitations.
—————
Following on from a request last year, the UEA would like to invite YOU to come TWICE to theirMovement and Exercise Laboratory (MoveExLab) to get involved with this Project if you can/if it’s appropriate for your circumstances.
Dr Balchin says: you never know how such involvement can directly or indirectly push your own rehab forward, at whatever time away from stroke you are. Knowledge is power, Anything that can give you clues and cues about the state of your rehab and current/future interventions can be useful.
Go for it if you can/if it’s appropriate for you!
Inclusion criteria: you need to be 18 or above, have had a stroke at any point in the past, be discharged from NHS stroke services and be without an allergy to latex.
What you’ll be doing:
Upon application, if no contra-indications are revealed, you’ll be invited to undertake 2 assessments at the MoveExLab.
These assessments (around 90 mins to complete each) will be between 2 and 4 months apart. In each, you’ll have EMG electrodes placed on your skin using hypoallergenic sticky tape. These will measure your muscle activity as you move and don’t hurt at all, but just record your natural muscle activity during movement.
They’ll then place reflective markers on your skin. These markers are tracked by infra-red cameras placed at the top of the walls of the MoveExLab.
You’ll then be asked to pick up a telephone several times, which is placed a number of different positions, whilst your performance on the tasks is recorded (and reconstructed on the computer).
Then you’ll complete some questionnaires about how you sleep.
Then you’ll wear a motion watch on each wrist for 7 days to measure your everyday activity, which you’ll then send back in an SAE.
No sort of ‘therapy’ is implemented to project participants.
The Team will be in contact with you throughout the period of your involvement.
Travel expenses can be reimbursed for return journeys of up to 50 miles (ie, 25 miles each way).
If you are travelling in from further away, you can claim travel expenses for your journey up to 50 miles in total as well.
—————-
Apply now by speaking with the principal investigator: Professor Valerie Pomeroy..
It’s probably true to say that a lack of motivation is one of the more serious factors involved in unsuccessful rehabilitations. A gradual diminishing of motivation is also a really normal reaction to setbacks, and stroke is one SERIOUS set-back.
You can bet that I’ve met quite a few stroke survivors over the years who’ve become prone to anxiety, depression and/or anger because of the condition they have found themselves in.
I hope that I’ve been able to facilitate at least some of these people towards the benefits of maintaining a ‘growth mindset’ concerning their recovery, despite their difficulties.
For example, there is a question that is often asked after a while if successes become imperceptible or grind to a halt. It is: ‘why bother to try retraining when nothing more seems to be happening, despite everything I’m doing so far?’
There are a number of instant answers that a neurologist would give you to this. Primary among them would be the point that even though changes may not be visibly occurring as a result of your efforts, your rehab training will still be as essential for warding off decline as well for driving positive functional change.This is why getting an ARNI trainer to tackle this with you is even more important.
So a good battle-plan is to find out more and more about your presentation (as it stands RIGHT NOW) and available treatments (AS THEY STAND RIGHT NOW), via as many knowledge-sources, is key.
For example, most people don’t understand (forget, aren’t told, or don’t read about the) need to continually promote an increase in active range of movement (AROM) in as many planes and pivots as possible.
Increase in non-functional AROM increases strength and muscle bulk, encourages muscular activity which promotes vascular return, decreases the potential for soft-tissue shortening and damage with resultant pain and stiffness and increases osteoblastic activity on your more-affected (and also possibly osteoporotic) side. Also, by doing this, you’ll render yourself more eligible for new technologies and/or medical options and emerging treatments to augment your retraining.
So, by steering you toward the potential inherent in effective retraining, I hope to promote a ‘growth mindset’ in you, if you’re not already ‘on-board’. You are a learner. And so am I, as a stroke survivor of what is now a full 25 years. You and I have to keep learning and keep retraining as stroke survivors, keep exploring and keep innovating over the long term. Easy to say, harder to do. But you MUST please, please write down a few things and start doing them. Then make a pattern of them day by day, which you don’t want to break, because it’s what you ‘do. And trust me, people will respect you for that.
Do MORE than able bodied people training-wise. Show them up!! Make them wish they WERE YOU!!
It’s possible.
Ultimately you may want to pass the things you’ve learned and constructed onto other survivors so that they can make of them what they will. I will show you how you can get motivated by getting successful; on what I call the ‘big fixes and the small steps’. This is, of course, only done by getting busy and starting to retrain with sensible staging posts. You’ll find your way through.
Have you thought about becoming an ARNI Stroke Rehab Instructor or nominating a colleague of yours to enter on the Course in order to Accredit/Qualify in Functional Rehabilitation After Stroke?
If not, please read on…. or please help if appropriate, by forwarding to a suitable colleague or two as a suggestion for consideration.
We have a couple of places left on forthcoming ARNI Stroke Rehabilitation Standard 6-Day Qualification Course… which is for the moment (due to Covid) available largely ONLINE.
Accredited by ARNI Institute, Middlesex University and very kindly assisted by the Institute of Neurology, UCL, and other experts in neurorehabilitation including from Oxford University. The Course has run 3 times per year for 15 years.
ARNI is well-known around the UK as a ‘go-to’ for stroke survivors and families when considering requesting an excellent instructor or therapist who will help survivors to rehabilitate in the community.
All dates are 10.15am – 5pm on Saturdays, for easiest access.
Day 1: January 22nd
Day 2: Feb 12th
Day 3: Feb 22nd
Day 4: March 12th
Day 5: March 26th
Day 6: April 9th
(Also practice training/shadowing days: March 22nd, April 1st, April 8th)
2. ADVANTAGES OF COMPLETION:
Learn how to really train stroke survivors: what they actually need from you in the community to recover as much function as possible.
Learn evidence-based skills, knowledge, retraining know-how and ‘tricks of the trade’ that you can offer and over again to stroke survivors (and families) to help them with ongoing rehab and self-management.
Be sent repeated referrals over time from ARNI Charity for rehab training.
Use the ARNI tele-rehabilitation system.
We may have people already on our lists who need your help, because we often have no other Instructor in specific areas to refer to or because existing Instructors sometimes find themselves unable to accept any more survivors to retrain.
Buy yourself or someone you care about some ARNI goodies TODAY: claim a huge 50% RIGHT NOW off any of the items featured below!
Get a bundle of ARNI gear at half-price – any published ARNI Book or manual (Successful Stroke Survivor or Had a Stroke, Now What?), physical DVD or DVD set, online anytime video subscription, limited edition blue 4-logo ARNI Training t-shirt, training diary, ARNI badged USB stick or cool gold-effect logo coaster!
3 DAYS ONLY! HURRY PLEASE! No orders in after 5pm on Friday 17th December please!
See Product page 1 and Product page 2 to see usual item prices and see below the illustration pictures for HOW TO GET THE ITEMS FEATURED BELOW at 50% off!
PLEASE NOTE:
We have no coupon facilities set up forthis Christmas offer, so just go to Product page here and choose everything you like that is featured on this page, note them down and then call us at ARNI on:
‘I’m pretty elderly now. If I have a stroke, I’m sure I won’t recover function’.
Good news though. This isn’t automatically so. The evidence reveals that overall, age is NOT considered to be a strong predictor of a better or worse functional recovery after stroke.
And elderly patients with stroke are still absolutely considered candidates for rehabilitation regardless of stroke severity, and each case needs to be considered on the basis of individual characteristics and potential. Factors such as fitness, cognitive functioning, family/community support and comorbidities (other health problems you may have had pre-stroke and may still have) are considered important in these cases.
Here is a wonderful photo of two people who are currently being retrained by ARNI Rehabilitation instructors: Harry Baker and his Grandfather! Harry, when he came to see us was just 15. His Grandfather is 95!
You probably know that stroke is most likely to occur after 55 years of age, with 38% of strokes occurring between 40-69 years and 59% of strokes occurring in people aged over 69 years. You’re most probably also aware that advancing age is considered a risk factor for stroke, with the incidence of stroke approximately doubling each year above 60 years of age. The average age of stroke is 72 years for men and 78 years for woman in the UK.
Although many people choose to ignore it, it’s very important for an older person to identify (or this being done for them by their GP) the things which increase their risk of having a stroke so that they can modify the way they live to reduce the risks.
The aging process is known to cause specific cardiovascular changes that impair heart and blood vessel function. These changes lead not only to reduced physical and mental ability, but aging is also a risk factor for cardiovascular disease (CVD). CVD is a classification term for diseases that involve the heart or blood vessels. For example: heart attack, stroke, heart failure, angina, hypertensive heart disease, rheumatic heart disease, cardiomyopathy, abnormal heart rhythms, congenital heart disease, valvular heart disease, carditis, aortic aneurysm, peripheral artery disease, thromboembolic disease and venous thrombosis.
A few lifestyle changes could reduce your risk.
Stopping smoking, reducing your alcohol intake, maintaining a healthy weight, eating healthier (high fibre, less fatty/surgery) foods and taking regular exercise can make a massive difference.
Existing medical conditions, like high blood pressure, high cholesterol, heart disease, diabetes, irregular heartbeat (atrial fibrillation), and having a transient ischaemic attack (TIA) can increase your risk of suffering a stroke. If you’ve not yet done so, you should probably ensure to consult your GP or a healthcare expert to summarise your risk factors for stroke as well as conduct a medication review for you.
Recovery after stroke
As noted above, older people are more likely to have pre-existing health conditions which can affect their ability to adjust to change and/or be the cause of functional limitations which in turn make ADLs more difficult to.
However, the brain has a life-long capacity to learn and adapt. Through processes called neuroplasticity and neurogenesis, the brain remodels itself in response to learning and experience. This allows the brain to change it’s structure and organisation; strengthening, adding or removing neural connections or creating new cells (neurons).
Neuroplasticity does decline as we age, but it doesn’t stop. It’s never to late to learn a new skill and many people use retirement as an opportunity to learn something new. This is only possible due the still present ‘plasticity’.
Does that mean that elderly stroke survivors can regain function after a stroke? Yes, and they do!
There is hope for recovery, even for elderly and previously ill stroke survivors. Specialist post-stroke care and early rehabilitation are key to gaining the best outcomes. Most improvements occur in the first 3 months after a stroke, after which they do slow down, but the brain will keep creating new neural pathways after this time: well after 6 months and in numerous cases, after many years. See how this is done in Had a Stroke? Now What? So it’s very important to begin and to continue with a tailored rehabilitation programme once no community (state given) help is available.
In order to bring about functional change, neural pathways for desired activities need to strengthened. At a very basic level, this can be optimally achieved through repetitions (facilitated by ‘smart’ use of use of some augmentations and principles which one can ‘add’ to movements to optimise their performance over time, always trying to work ‘on the edge of your current ability. How do do this is explained in my ‘stroke rehab possibilities wheel diagram’ in Had a Stroke? Now What?. The more repetitions you can achieve in a shorter time, the better the brain can re-structure. The skill you are trying to ‘re-learn’ should be something that is relevant and meaning for you.
You’re more likely to succeed if you deem the task or tasks important and worth-while. For this reason, I’ll show you how you can set mini-plans (or goals) and identify what you want to achieve, so that you can prioritise your time. This is particularly important if you suffer from fatigue and low energy levels. Goal-setting (although to many people it sounds like a very woolly term) will help you to stay motivated and on-task if you match it with record-keeping. Actually, record keeping is the valuable one. Goals can quite vague but recording what you achieve each time you retrain is the massive biggie. So few people really do it, and it’s a shame. They really should – success lies in knowledge – knowledge is power!
So, young or old – let’s go! There’s ALWAYS a way. If you can’t locate what that way is at the moment, ask us and we’ll give you some pointers ok?
To get involved with rehab talk with other stroke survivors, please visit ARNI Facebook
The majority of stroke survivors whom I’ve met, when describing their prior physiotherapy and any other rehabilitative efforts, will report that the focus of therapy was usually on seated stabilisation, seat to stand, weightbearing and walking practice. All vital stuff. But only a small minority remembered being introduced to/practising upper limb exercises.
This happens for a number of reasons, but as time and resources are most usually limited, therapists often do not have time to devote to extensive hand-function efforts. Many receive no upper limb therapy at all. And by the time further treatment is sought, the task is all the more harder. At the height of the pandemic, many patients were told that it was safer to go home and receive no therapy or no further therapy.
This is why it’s critical that the leading edgeUpper Limb Clinicdeveloped at the Institute of Neurology at UCL by Professor Nick Ward builds up more and more a body of evidence of efficacy so that it becomes clear that a ‘3 week intensive blast’ of multi-therapies that such a Clinic can offer, with the learning for survivors and families that can accompany it, can become an effective bolt-on or plug-in funded for each hospital in the UK with a stroke unit in order to push/promote/kick-start recoveries. Maybe this will happen in due course. I hope so!sive
In the meantime, it’s vital that stroke survivors are shown what to do as far as upper limb is concerned in the community, as soon as possible after discharge, in order to continue the work of the therapists or initiate it if none has yet been done.
The reason is that all evidence points to the fact that high dosages of repetitions, over time, stand best chance of assisting upper limb recovery. This has to be done by the survivor, at their own residence. Survivors need to know what to try to do themselves and what they need to seek help with/for.
The evidence (see yearly-updated in-depth reviews of well over 4,500 studies including over 2,170 randomized controlled trials at www.ebrsr.com) reveals that:
Task-specific training, alone or in combination with other therapy approaches, may be beneficial for upper limb function.
Higher and lower intensity task-specific training may have similar effects on upper limb function.
Trunk restraint with reaching training may improve upper limb function.
Let’s discuss how you as a stroke survivor can use this evidence. Remember, high dosages of repetitions (of reach, grasp and release) are needed. Remember that all attempts at repetitions (including mental practice) drive neuroplasticity. You NEED to get it done, over and over again, even if nothing is happening: there are ‘tricks of the trade’ as it were’ that you can use.
I’m going to show you all of this in a series of Youtube clips.
Have a look at this small video I put together: this is clip 1 of 20 or so about upper limb training. Then take part with me by subscribing to the new ARNI Stroke Rehab Tips on Youtube. Upper limb rehab will come first and Video 1 is already up on there: watch and subscribe for further Youtube videos! Many other stroke rehab topics will be loaded up on there as time moves on.
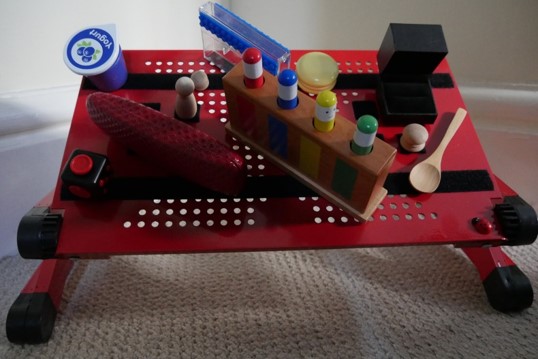
If you do want to take part, you need only a minimum amount of kit. A short stick (cut a broomstick and chamfer the edges), a tray or book, some items with blue tack stuck to the bottom (or MUCH better a laptop board with heavy duty Velcro strips attached and some specific items with Velcro squares attached to them – click the link to get, or make your own board).
Being in a seated position is fine when doing upper limb task-specific training. But completing the reaching task by moving your trunk forward to complete a reaching activity is ‘cheating’. This is where trunk constraint works well.This is often done via a chest seatbelt/harness.
How to start retraining your upper limb after stroke? Your starter programme consists both of stretches and tasks. You may or may not have been taught how to safely self-stretch but the idea is that more is better and safety is paramount. You have to stretch your upper limb (gently), knowing at the same time simply stretching won’t bring recovery. You have to be task-focused. So, when you do a stretch, you then do something challenging and specific functionally with the stretch.
For example, stretch, then try to pick a hairbrush up and put it into a cupboard. In your retraining sessions, stretches must be considered as promoting the chances of the successful performance of the task.
Remember my upper limb catch-phrase: stretching enables the task and extends ‘time on task’.
These are very important for improving your potential ability to reach for, grasp and release items with your hand: activities that are denied to so many stroke survivors. You can use stretches daily in order keep muscles long and prevent further complications. The best results are often seen in people who have consistently stretched their wrist, fingers and thumb on their more-affected side from a very early period in the hospital.
Upper limb task-specific practice concerns reaching (which you perform mainly with your shoulder, elbow and wrist joints) and grasping/releasing (which you do mainly with your fingers and thumb joints). Stroke survivors often find it very hard to make purposeful movements requiring precise control of either; rendering movement slow, inaccurate, and usually not well directed or coordinated. Isolated recovery efforts for the upper limb, often in terms of grasping and releasing an item during a task, correspondingly demand effort and accuracy.
Unlike (to an extent), lower body, training coping strategies for and during rehabilitation of the upper limb should be largely avoided.
If you have spasticity and find it hard to reach away from your torso, you may tend to ‘throw’ your more-affected arm at a task mainly by activating your shoulder joint. This stands in contrast to a more controlled movement sequence, where your arm can move away from your torso using your shoulder, elbow and wrist joints to help position your hand to complete a task. The latter situation is better than the former.
Success at reaching therefore needs to be trained for. Building up strength and working for incremental spasticity decline can be worked on at the same time. So, trunk constraint whilst performing task-practice has strong evidence for improving outcomes, because it makes ‘cheating’ nearly impossible to do.
Also, limb de-weighting via wrist holding or using de-weighting technology is a therefore a good way of facilitating this from the start. See picture, below and left. This is because ‘heavy arm’ can render tasks very difficult to perform.
I’ll show you all this in one of the videos, and how a therapist, trainer or any family member can do this precisely to help the survivor ‘get the ‘gap’ between thumb, first finger and middle finger, in order to pick up an object.
So, arm de-weighting, often in terms of assisting in reaching for an item during a task can be used to initiate and/or extend your time practising a task.
One thing you need to know is that although there is evidence that functional control of your hand will only improve once you gain more control over joints which are closer in towards the body (proximal) rather than further away (distal), recent evidence suggests that you should be also be trying to work with your fingers and thumb right from the start rather than waiting for your arm to get stronger in order to position your hand accurately.
This might sound strange if you can’t even ‘get a gap’ between your first finger and your thumb, or that your fingers and thumb are ‘floppy’. Both states would seem to make ‘useful’ hand function non-existent.
However, it’s suggested that, via specific retraining, distal control can and should be trained for immediately after stroke, This is also because if you waited for control to return from proximal to distal, you might achieve some strength in the shoulder, elbow and wrist over time but may not have done any task-specific grasp and release attempts at all, let alone put in the very large amount of intensive retraining time that might stand a chance of helping you regain control of the main reason why you have an arm in the first place.
Being physically active is a great way to improve and maintain health and wellbeing… and reduce the chance of a stroke. And of course, rehab is required if you’ve had one.
If you have had a stroke, you will hopefully have been shown how to implement your own programme of consistent repetitive movement at home during your recovery.
To help you with this and many other features of tackling limitations from stroke, you are invited to take part in a week-long programme of online sessions.
Each has been designed to encourage open dialogue and activity between researchers, clinicians, charities and stroke survivors.
The Programme of Events starts with discussion about how researching the brain post-stroke leads to better health outcomes and ends with a workshop about staying active after stroke.
As usual, I’ll be running a workshop.
This will be on Tuesday 26th October from 3.30pm to 4.30pm.
I’ll be showing you some video clips (concerning recovery of the upper limb) and attempt to guide you through some simple methods to encourage recovery of reach, grasp and release via repetitive task-activity.
Each survivor has their own particular presentation and we’re going to see what we can do so that everyone receives helpful tips for progression
If you like, to prepare, do get a few implements together in a pile (like chess pieces) and stick some blue-tack on the bottom of each one. Or (as I’ll be teaching using this simple task board in order to demonstrate), do feel free to get hold of one. Or of course, make your own!
You’re warmly invited to participate! Let’s do it!!
We’ll also be joined by the team behind the campaign We Are Undefeatable, which aims to inspire and support people with long-term conditions to build physical activity into their lives in a way that works for them. They will talk about their campaign, the kind of movements that can be done from the comfort of your own home, and give some tips about how to make being more active fun.
The impact so far of the Prescription, and its potential, will be assessed by four leading names from across neurorehab. The webinar, held by NR Times working alongside NRC Medical Experts, is the first in a series to analyse key issues in neurorehabilitation. The panel taking part in the webinar are:
Professor Mike Barnes, one of the UK’s most experienced neurorehabilitation experts
Hokman Wong, senior solicitor and brain injury specialist at Bolt Burdon Kemp.
The Rehabilitation Prescription is designed to give patients, GPs, case managers and everyone involved in an individual’s care a comprehensive overview of their immediate and longer-term neurorehabilitation requirements in one summary document, which acts as a guide to navigate the complexity of neurological disability.
The event will look at whether the Rehabilitation Prescription really is improving patients’ lives or whether, when the patient reaches the community, outside of the realm of NHS help, a rehabilitation prescription that can be used to guide ongoing rehabilitation, is part of standard current practice or not.
Certainly, rehabilitation prescriptions for stroke survivors which are updated as a patient advances in their don’t seem to happen at all. But it it would be invaluable for a patient to know that any therapist they work with can access a ‘passport’ containing up to date information on their rehabilitation needs, which can perhaps also be updated over time…
* The webinar is free to attend but registration is needed. There is also the opportunity to submit questions in advance. To register, visit here.
Your exclusive invitation for professionals who help those with brain injury, and for survivors and their families, only by application RIGHT NOW!
For 2.5 hours, this Thursday (23rd September 2021, 10.30am to 1pm), listen to and talk directly with the UK’s Leading Experts in Stroke Recovery.
Listen to and ask Professor Val Pomeroy (University of East Anglia) about getting to grips with/analysing action control and Professor Avril Drummond (University of Nottingham) about managing fatigue.
Co-chairs: Hokman Wong (Bolt Burdon Kemp) and Tom Balchin (ARNI).
This is a rare chance for you to ask these two engaging experts about their fields and any other query you have. They will present for 45 mins each and the rest of the time will be concerned with taking your questions. So do come prepared with a few questions to ask: go for it!
There is NO CHARGE and we can also also apply on your behalf for a Certificate for 2.5 hours National CPD Service CPD points for attending.
These people are experts who I myself try and engage with when I need help in order to help a patient with a certain issue. So whoever you are, be it professional, survivor, family member or carer, do book up for this event (see flyer below).
Reservations for Thursday’s awesome event are going quickly, so please do read the flyer below and reserve yours NOW by emailing tom@arni.uk.com
Please note: if you already registered (for example, you attended last Thursday’s Conference with Professors Cathy Price and Heidi Johansen-Berg), then there’s nothing more to do except login at 10.15 or so, ready for 10.30 start!
Professor Valerie Pomeroy is Professor of Neurorehabilitation and Director of Research at the School of Health Sciences, University of East Anglia with expertise in translational research into neuroscience-based rehabilitation interventions (proof-of-concept and early phase trials). Emphasis is placed on care closer to home and development of sensitive physiological measures for timely identification of response to therapy, prediction of response and the neural correlates of response. A particular expertise is in MedTech development especially after securing team mentorship on the Design Council Leadership Programme in 2014.
Professor Avril Drummond is Professor of Healthcare Research in the School of Health Sciences in the University of Nottingham. She is Non-Executive Director at University Hospitals of Derby and Burton NHS Foundation Trust. She is particularly interested in patient care and NHS research. She is an expert in rehabilitation research and evaluation of service delivery. An occupational therapist by background, her research includes rehabilitation research in stroke, traumatic brain injury, low back pain, total hip replacement, Multiple Sclerosis, specific studies of GP fit notes, hemianopia, early supported discharge, fatigue, falls prevention and home visit assessments, the work of the stroke units and community re-enablement.
Zoom based ARNI Instructor training course; starts on September 20, 2025
ARNI runs the ONLY FUNCTIONAL REHABILITATION & EXERCISE TRAINING QUALIFICATION CURRENTLY AVAILABLE IN THE UK which teaches experienced therapists and exercise instructors how to continue the rehabilitation path of stroke and other acquired brain injury survivor.
You will learn how to teach things that stroke survivors really want, and will ask you for help with. With this CPD you will be ready to meet the full needs of a referred client.
Functional rehabilitation & exercise training after stroke taught by ARNI is characterised by: essential upper and lower limb task practice in order to recover action control, innovative physical coping strategies in order to perform ADLs independently… and appropriate stroke-specific cardiovascular and resistance training.
Cardiovascular exercise is defined as any type of exercise that gets your heart rate up and keeps it up for a prolonged period of time. It isn’t difficult to do and there are lots of options.
Walking, jogging, running, cycling, stepping, swimming, boxercise and rowing are examples for those who haven’t suffered a stroke. Options for stroke survivors are narrowed somewhat from these choices but at least one or other of the above can probably be achievable, either supported or unsupported.
When you do these types of activities, your respiratory system starts working somewhat harder as you begin to breathe faster and more deeply. Your blood vessels expand to bring more oxygen to your muscles, and your body releases natural painkillers (endorphins).
exercises like walking and swimming, which can be done with friends or family, are a great way to socialise while achieving some exercise. Sometimes you won’t be able to get out and about as often as you need, to do a form of exercise , so it’s a good idea to plan how you’re going to get it done by yourself at home. www.arni.uk.com
You've heard of Tai Chi, yes? And the moderate to strong evidence for in assisting functional recovery from stroke? And Ki-gong (or Qigong, qi gong, chi kung, chi 'ung, or chi gung - same things)? In essence, for stroke survivors, I think it's better than Tai Chi because it's a pretty static (and v powerful) system of coordinated body-posture and movement, breathing, and energy-focus/production. I practiced it extensively in my own acute to chronic recovery (I basically bought a couple of books and taught myself how to do it - and did it - every day without fail). I used Wong Kiew Kit's book - and he's done lots more since - see Amazon, PLEASE INVESTIGATE IT - watch some youtube vids and then get outside or even next to an open window if it's raining - and do it! V good for balance, gait control and upper limb - all-round proprioception recovery, really...
A systematic review and meta-analysis of randomized controlled trials on the effect of Qigong exercise on motor function in stroke patients has just been published (25 Jul 2023) in the Journal 'Topics in Stroke Rehabilitation'
Methods: Randomized controlled trials that evaluated the effect of Qigong on motor function of stroke patients were obtained from PubMed and Chinese National Knowledge Infrastructure through May 2022. Mean values and standard deviations of the post-intervention score in both experimental group and control group were collected to calculate the mean difference (MD) and corresponding 95% confidence interval (95% CI) of each study, which were quantificationally summarized using the Review Manager 5.3 software.
Results: Nineteen randomized controlled trials enrolling 1487 stroke patients were included. Pooled results indicated that Qigong exercise had beneficial effect on balance function (Berg Balance Scale), limb motor function (Fugl-Meyer Assessment); upper limb, lower limb and walking function (6-min walking test) of stroke patients. It was also found to be associated with an improvement in trunk function as indicated by the Trunk Impairment Scale.
Motor impairment is one of the most common defects after stroke, which could seriously affect the life quality of stroke patients. Exercise intervention gradually becomes a popular alternative reha...
How does ARNI work? Current neurological scientific research supports the premise that your brain has the ability to positively adapt to assist recovery of lost function after stroke. Probably one of the biggest advantages you have as a stroke survivor is your brain’s astonishing capacity for neuroplasticity, (Ask your current therapist about it). The notion of brain plasticity is one of the most extraordinary discoveries of the twentieth century. It suggests that the location of a given function in the brain (for example, speech) can move to another area of the brain. In the case of stroke, brain plasticity refers to healthy brain cells taking over the functions of damaged brain cells. This means that certain lost functions, such as speech and language, may re-emerge as the result of intensive rehabilitation. The idea of the brain being able to ‘adapt’ to a traumatic event is new and optimistic.
So, why is that more people are not getting more movement back again after stroke? The number one reason is physiological. For instance, stroke causes a number of changes with the body that must be tackled incrementally because stroke survivors frequently have insufficient underlying motor activity to start the kind of task related practice they need to do.
This system contains an abundance of techniques which are designed to prime the body for task-related practice. Often, therapists help stroke survivors to get to their feet and walk again after brain injury and many achieve great successes in the very short time they have to work with them in the acute/chronic stages. However we often see stroke survivors who find it hard to move on from sticks and orthotics… and other aids to functional movement and many feel they can achieve better function in their paretic (weak) hand if given a chance to do so. We can help in this situation.
With your ARNI Instructor: The system you are about to learn has been refined over a period of 24 years with stroke survivors of varying ages, type and severity of stroke… and of time from injury. With your trainer, the application of individual trial and error is required in order to see what can be done using the specialised ARNI rehabilitation exercises and strategies… and to understand what goals can be reached. All training given will be appropriate to the individual, even though you may be working in a group class.
With your trainer, the application of individual trial and error is required in order to see what can be done using the specialised ARNI techniques and to understand what goals can be reached. You need to be working ‘on the edges’ of your current ability to stimulate maximum neuroplasticity.
Your Instructor will show you progressively more advanced exercises including an introduction concerning how you can prepare your body for rigorous weight training, if that is a further goal of yours. Usually only body-weight resistance work is used by Instructors, although the ARNI training syllabus incorporates just 2 highly effective techniques for compound resistance training (the deadlift and squat). Both are unusual variations of the usual techniques, as we have adapted them for stroke survivors’ limitations.
Your training will finish when you find you no longer need the help of our specialists, but you can continue to use their gyms or training areas, or find another outlet in your own area, however old you are, to continually be active in order to maintain and add to your gains in terms of movement, stability, strength and conditioning. HARD WORK? Well, yes…
You might find yourself wondering by now whether you could even think about doing something like this especially as we will tell you it requires a lot of hard work. Actually it is progressive hard work. There is a big difference. We will surely push you, but within your own limitations, which are of course going to be moving targets.
The rehabilitative movements are done at a very basic level, designed especially for the trainee to understand how THEY can start to take charge of increasing action control (eg., enhance balance, reduce spasticity in upper limb, control the effects of drop-foot) Likewise, essential fitness and resistance training is carried out at a low level with great care in exercise selection and attention to form. This is NOT treatment by passive positioning. This is you DOING it. This is you using your plastic brain and regaining movement. Call ARNI on 0203 053 0111; or email support@arni.uk.com www.arni.uk.com #strokerehabilitation #strokerehab#strokerecovery#arnistrokerehab#neurorehab#neuroplasticity#neurorehabilitation #strokerecoveryexercises #strokeexercise#exerciseafterstroke#strokesurvivors... See MoreSee Less
Just to remind you - The ARNI programme offers a tailored training regime for each individual, which revolves around functional movement with task-related exercises. ARNI will teach you the importance of encouraging brain plasticity with the practice that you do. The ARNI Approach is the first comprehensive collection of reality-based techniques grounded in contemporary neurological research perspectives that is available for you to access after the assistance of the therapist.
This dedicated approach is completely unique; it has been designed specifically for the needs of the stroke survivor with partial paralysis who feels that they cannot find any way to recuperate further using more traditional approaches. It relies on the effects of a combination of neurologically complementary strategies.
Traditional therapy has for many years now been challenged by evidence revealing that task specific strength training and exercises.
The ‘ARNI Approach’ is an exciting development in the field of stroke rehabilitation, that has an international reputation for serious results in terms of it ability to assist stroke survivors to�...
So, walk round your house, walk outside if you can; depending on your environment, try building up distances, or count to 10 steps, turn around and go back. It is important as a stroke survivor that you don’t use your lack of mobility as an excuse for immobility. Don’t stop at just walking in a straight line either. Walk around an imaginary circle on the floor. Do lots of these. Stop, turn, and walk around the other way. Then repeat without losing your balance. Even experiment with one or two backwards steps, but only one or two! www.arni.uk.com #neuroplasticity#strokerecovery#arnistrokecharity #ARNIstrokerehab#neurorehab#arnistrokerehab #arnistroke#strokerehabilitation #ARNIstroke #walkingafterstroke... See MoreSee Less
It’s important to set realistic goals during stroke recovery; and keep setting higher goals as you progress. The more you improve, the more you are able to set new goals for a higher level of recovery.
If you like this post then please share it with others. Each time that you share a post, you can directly help other people – as who knows which people in the world might find us and gain, either directly from the charity or simply by being able to copy an ‘innovative and useful’ move/trick of the trade that might help them manage after stroke.

 Tiredness is something we all experience in our everyday lives. But how about the sort of tiredness which seems to be unrelated to physical or mental exertion, and does not seem to be alleviated by rest? This is a real problem for many stroke survivors on top of the many other problems they may face – and is called ‘fatigue’.
Tiredness is something we all experience in our everyday lives. But how about the sort of tiredness which seems to be unrelated to physical or mental exertion, and does not seem to be alleviated by rest? This is a real problem for many stroke survivors on top of the many other problems they may face – and is called ‘fatigue’. The Effort Lab, led by Dr Anna Kuppuswamy, based at the Institute of Neurology, UCL, in London, has been studying fatigue over the last 10 years to better understand the brain mechanisms that underlie this highly debilitating symptom, not only after Stroke but across other neurological conditions such as Multiple Sclerosis and Parkinson’s Disease.
The Effort Lab, led by Dr Anna Kuppuswamy, based at the Institute of Neurology, UCL, in London, has been studying fatigue over the last 10 years to better understand the brain mechanisms that underlie this highly debilitating symptom, not only after Stroke but across other neurological conditions such as Multiple Sclerosis and Parkinson’s Disease. It takes no more than 45 minutes on an online combined quiz and questionnaire:
It takes no more than 45 minutes on an online combined quiz and questionnaire: 
 Strong evidence exists that physiotherapy improves the ability of people to move and be independent after suffering a stroke. But at six months after stroke, we know that many people remain unable to produce the movement needed for every-day activities such as answering a telephone. So, what can be done?
Strong evidence exists that physiotherapy improves the ability of people to move and be independent after suffering a stroke. But at six months after stroke, we know that many people remain unable to produce the movement needed for every-day activities such as answering a telephone. So, what can be done? 2. Second, to optimise a physiotherapist’s chances to advise/work on an optimal combination of rehab interventions for each individual after stroke, it would be ideal to find out what kinds of sleep patterns are most beneficial for them.
2. Second, to optimise a physiotherapist’s chances to advise/work on an optimal combination of rehab interventions for each individual after stroke, it would be ideal to find out what kinds of sleep patterns are most beneficial for them. Ideally, more portable equipment should also be able to be accessed by therapists, which would cost less and is designed for use in small spaces. But such equipment would have to also be sensitive enough to provide meaningful feedback for therapists in a similar way to those used by the specialist labs. Such feedback could then be very useful for therapists and survivors to create optimal rehab plans together which would really enable the survivor to work on his/her edges of current ability.
Ideally, more portable equipment should also be able to be accessed by therapists, which would cost less and is designed for use in small spaces. But such equipment would have to also be sensitive enough to provide meaningful feedback for therapists in a similar way to those used by the specialist labs. Such feedback could then be very useful for therapists and survivors to create optimal rehab plans together which would really enable the survivor to work on his/her edges of current ability. A School of Health Sciences research team at the University of East Anglia (UEA) headed up by
A School of Health Sciences research team at the University of East Anglia (UEA) headed up by 
 Go for it if you can/if it’s appropriate for you!
Go for it if you can/if it’s appropriate for you!
 They’ll then place reflective markers on your skin. These markers are tracked by infra-red cameras placed at the top of the walls of the MoveExLab.
They’ll then place reflective markers on your skin. These markers are tracked by infra-red cameras placed at the top of the walls of the MoveExLab. 


 You can bet that I’ve met quite a few stroke survivors over the years who’ve become prone to anxiety, depression and/or
You can bet that I’ve met quite a few stroke survivors over the years who’ve become prone to anxiety, depression and/or  I hope that I’ve been able to facilitate at least some of these people towards the benefits of maintaining a ‘growth mindset’ concerning their recovery, despite their difficulties.
I hope that I’ve been able to facilitate at least some of these people towards the benefits of maintaining a ‘growth mindset’ concerning their recovery, despite their difficulties.
 Do MORE than able bodied people training-wise. Show them up!! Make them wish they WERE YOU!!
Do MORE than able bodied people training-wise. Show them up!! Make them wish they WERE YOU!!
 Accredited by ARNI Institute, Middlesex University and very kindly assisted by the Institute of Neurology, UCL, and other experts in neurorehabilitation including from Oxford University. The Course has run 3 times per year for 15 years.
Accredited by ARNI Institute, Middlesex University and very kindly assisted by the Institute of Neurology, UCL, and other experts in neurorehabilitation including from Oxford University. The Course has run 3 times per year for 15 years. All dates are 10.15am – 5pm on Saturdays, for easiest access.
All dates are 10.15am – 5pm on Saturdays, for easiest access. Please enquire.
Please enquire. 



 A few lifestyle changes could reduce your risk.
A few lifestyle changes could reduce your risk.
 In order to bring about functional change, neural pathways for desired activities need to strengthened. At a very basic level, this can be optimally achieved through repetitions (facilitated by ‘smart’ use of use of some augmentations and principles which one can ‘add’ to movements to optimise their performance over time, always trying to work ‘on the edge of your current ability. How do do this is explained in my ‘stroke rehab possibilities wheel diagram’ in
In order to bring about functional change, neural pathways for desired activities need to strengthened. At a very basic level, this can be optimally achieved through repetitions (facilitated by ‘smart’ use of use of some augmentations and principles which one can ‘add’ to movements to optimise their performance over time, always trying to work ‘on the edge of your current ability. How do do this is explained in my ‘stroke rehab possibilities wheel diagram’ in 
 Being in a seated position is fine when doing upper limb task-specific training. But completing the reaching task by moving your trunk forward to complete a reaching activity is ‘cheating’. This is where trunk constraint works well. This is often done via a chest seatbelt/harness.
Being in a seated position is fine when doing upper limb task-specific training. But completing the reaching task by moving your trunk forward to complete a reaching activity is ‘cheating’. This is where trunk constraint works well. This is often done via a chest seatbelt/harness. Remember my upper limb catch-phrase: stretching enables the task and extends ‘time on task’.
Remember my upper limb catch-phrase: stretching enables the task and extends ‘time on task’. If you have spasticity and find it hard to reach away from your torso, you may tend to ‘throw’ your more-affected arm at a task mainly by activating your shoulder joint. This stands in contrast to a more controlled movement sequence, where your arm can move away from your torso using your shoulder, elbow and wrist joints to help position your hand to complete a task. The latter situation is better than the former.
If you have spasticity and find it hard to reach away from your torso, you may tend to ‘throw’ your more-affected arm at a task mainly by activating your shoulder joint. This stands in contrast to a more controlled movement sequence, where your arm can move away from your torso using your shoulder, elbow and wrist joints to help position your hand to complete a task. The latter situation is better than the former. Also, limb de-weighting via wrist holding or using de-weighting technology is a therefore a good way of facilitating this from the start. See picture, below and left. This is because ‘heavy arm’ can render tasks very difficult to perform.
Also, limb de-weighting via wrist holding or using de-weighting technology is a therefore a good way of facilitating this from the start. See picture, below and left. This is because ‘heavy arm’ can render tasks very difficult to perform.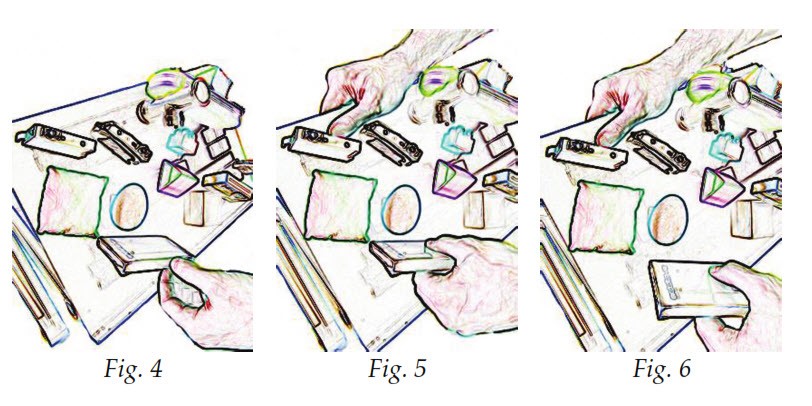 This might sound strange if you can’t even ‘get a gap’ between your first finger and your thumb, or that your fingers and thumb are ‘floppy’. Both states would seem to make ‘useful’ hand function non-existent.
This might sound strange if you can’t even ‘get a gap’ between your first finger and your thumb, or that your fingers and thumb are ‘floppy’. Both states would seem to make ‘useful’ hand function non-existent.
 The UCL World Stroke Day Forum is back!
The UCL World Stroke Day Forum is back!  To help you with this and many other features of tackling limitations from stroke, you are invited to take part in a week-long programme of online sessions.
To help you with this and many other features of tackling limitations from stroke, you are invited to take part in a week-long programme of online sessions.  Each survivor has their own particular presentation and we’re going to see what we can do so that everyone receives helpful tips for progression
Each survivor has their own particular presentation and we’re going to see what we can do so that everyone receives helpful tips for progression